Many thanks to Andrew Snyder-Beattie and Joshua Monrad for their feedback during this project. This project was completed as part of contract work with Open Philanthropy, but the views and work expressed here do not represent those of Open Philanthropy. All thoughts are my own.
My full spreadsheet with results and calculations can be found here.
Summary Statistics
- I adopt a loose and arbitrary definition of biosecurity where I am primarily concerned with interventions aimed at preventing or mitigating the effects of disease outbreaks. This especially includes interventions targeting or suitable for global catastrophic biological risks (GCBRs).
- Given this definition, biosecurity roughly represents 1.3% of the global spend on public health or about $130bn of $10tn a year.
- Of this $130bn, governments likely make up to $100bn (80%) as an upper bound, and the actual figure could be much lower. The US government is likely the biggest government spender, spending $24.3bn in 2023. Private philanthropy is likely about $1bn (1%). The rest comes from private spending, private philanthropy, and public-private partnerships that aren't independent foundations (e.g., universities).
- However, the vast majority of biosecurity spending goes towards vaccine development, disease surveillance, and pathogenesis research. My impression is that areas such as next-gen PPE, far-UVC, and research into GCBRs do not receive much philanthropic funding at all outside EA. EA players likely represent roughly 4% of biosecurity philanthropic funding.
See ‘Results’ for more information.
This was scrappily put together in no more than 40 hours of work and very little expert consultation, so I note extremely high levels of uncertainty in these figures, although I would estimate they are correct within a factor of 2-3 given the conception of biosecurity with a reasonable degree of confidence (~70%). However, my uncertainties are much wider when I factor in uncertainties about what constitutes 'biosecurity' to begin with (closer to a factor of 5 with the same degree of confidence, with the upper tail being much higher).
About
I’ve spent some time recently trying to understand exactly how well-funded is ‘biosecurity’ philanthropy.
An important caveat is that ‘biosecurity’, in its broadest sense, is “the prevention of disease-causing agents entering or leaving any place where they can pose a risk to farm animals, other animals, humans, or the safety and quality of a food product”. Under this definition, the space of biosecurity interventions is exceptionally broad: safe food handling and storage practices, screening imported produce, waste management, proper sanitation, and the use of HVAC systems are all biosecurity interventions.
Instead, I’m mostly interested in a subset of interventions largely aimed at preventing or mitigating the effects of disease outbreaks. This especially includes interventions targeting or suitable for global catastrophic biological risks (GCBRs) such as pathogen-agnostic early detection, vaccine platform technologies, and regulating the use of nucleic acids through methods such as DNA synthesis screening. However, a number of interventions not primarily targeting GCBRs may still have quite large consequences for them. Antimicrobial resistance likely contributes towards millions of deaths a year; is a desired property of any maliciously designed pathogen, and techniques for detecting antimicrobial resistance are essentially the same techniques we would use for detecting novel pathogens. I think it is plausible that much work on influenza, research into the pathogenesis of pathogens, and a number of national security interventions are additionally relevant to pandemic prevention and mitigating GCBRs amongst a number of interventions.
The upshot is that trying to delineate the boundaries of ‘biosecurity’ simpliciter, ‘pandemic prevention’, or ‘GCBR-relevant biosecurity’ is a doomed project. Additionally, I think attempting to do so can often lead to the dangerous exclusion of important considerations, technologies, and programs that do not obviously fit into one’s chosen frame.
However, I think the benefits of understanding how well biosecurity is funded; the distribution of funding across different types of actors, and how biosecurity funding is split across interventions is highly important for the efficient allocation of resources on the margin. In turn, whilst I don’t think we can be very confident about attempts to do so, I think the potential insights to be gained from trying outweigh the high levels of uncertainty.
Why Does This Matter?
Biosecurity is constituted by exceptional heterogeneity. Two prima facie identical interventions can have remarkably different consequences depending on the specific threat model, pathogens of concern, geographical context, and a number of contingencies. A wastewater surveillance program targeting an intentionally engineered stealth pandemic in a country where wastewater treatment is prevalent is much more likely to succeed than a wastewater surveillance program targeting zoonotic diseases with a high case fatality rate in a country with scarce wastewater treatment.
Without relatively strong priors about the probability distribution of threat models, pathogen characteristics of concern, pandemic intensities, and all manner of practical considerations, I am generally pessimistic about the value of comparing and contrasting different biosecurity interventions on the margin. At the very least, I think there should be very clear bounds and scope restrictions for this type of modelling. In turn, I would not suggest that current funding levels are a reliable proxy for how saturated interest in specific biosecurity interventions is.
However, I do think order-of-magnitude differences can teach us a lot about biosecurity philanthropy and biosecurity more generally, as well as effective altruism’s (EA) place within it. Some of these questions worth answering might be:
- How large is biosecurity philanthropy as a proportion of total spending on biosecurity?
- How large is biosecurity philanthropy compared to public health philanthropy?
- Who are the biggest funders within biosecurity? What are their concerns?
- Are there any significant differences in the funding priorities or focus areas among the leading biosecurity philanthropists?
- Where is most biosecurity funding coming from geographically?
- What are the primary areas of interest within biosecurity philanthropy?
- How well-represented are EA concerns (especially relating to GCBRs) within biosecurity philanthropy?
I focus on biosecurity philanthropy largely because it is less visible than government spending on biosecurity, which the United States likely dominates (see Part III: Biosecurity BOTECs). However, I think understanding the biosecurity philanthropy landscape may also be more decision-relevant for organisations and individuals in EA seeking to attract and divert funding towards the most high-impact causes.
Methodology
I ended up focusing on three mini-investigations:
- Who are the philanthropic funders in biosecurity and how much do they spend in a year?
- How does this biosecurity spending breakdown by intervention?
- How well-funded is biosecurity?
I spent roughly 40 hours on this (excluding this post), with the majority of this (~34h) being on Part I; ~3h on Part II, and ~3h on Part III).
Part I: Biosecurity Spending by Foundations
Part I involved searching through a long list of foundations and producing (often very scrappy) estimates of lower and upper bounds of how much they spent on biosecurity.
1. Structured Search
Firstly, I ended up focusing on this list of search tags (and some minor variants):
- Technologies of Interest
- Next-Gen PPE
- Far-UVC
- Rapid Vaccines
- Metagenomic Sequencing
- AI-Bio
- Key Areas
- Global Catastrophic Biological Risks (GCBRs)
- Bioweapons
- Bioterrorism
- Dual-Use Research of Concern
- Lab Leaks
- Novel Pathogens
- Pathogenesis Research
- Biosecurity Policy
- Gain of Function Research
- Indoor Air Quality
- Lab Biosafety
- Other Search Tags
- Biosecurity
- Biodefense
- Antimicrobial Resistance
- Influenza
- Infectious Disease
- Disease Surveillance
These were exhaustive of the areas I ended up defining as ‘biosecurity’. For the reasons given in ‘About’, this is a very scrappy delineation that represents the technologies, problems, and considerations I felt were most connected to preventing or mitigating the effects of disease outbreaks, especially GCBRs. For each of these, I then searched them against the following search items and the word “Funding” on Google.
- Grant
- Trust
- Donation
- Initiative
- Foundation
- Fund
- Philanthropy
The full format of my searches was ‘[Key Word]'"[Search Item]'" Funding’. For each search, I looked at the first 5-10 pages on Google and noted any foundation that came up.
2. Grantee Search
I additionally looked through a number of organisation websites and annual reports to see if they state who their funders are. These included organisations who report their funders such as 1DaySooner, the Johns Hopkins Center for Health Security, the Centre for Long-Term Resilience, UNIDIR, and Preventing Future Pandemics. The purpose of this step was largely to fill in the gaps from my structured search, hence it was a lot more ad hoc.
3. Foundation BOTECs
This was by far the most involved part of this entire investigation and ended up taking two iterations. Ultimately, for every foundation, I attempted to produce a plausible lower-bound figure for how much they were spending on biosecurity in a given year and a plausible upper-bound. My overall estimate was, therefore, just the mean, unless I felt I was able to collect more high-fidelity data.
In the initial iteration, the most useful tools were either foundation annual reports or grant databases. Organisations like the Burroughs Wellcome Fund produce annual reports that give relatively detailed breakdowns of their spending in different areas. Organisations like Open Philanthropy provide data on individual grants.
For actually estimating lower and upper bounds, I didn’t really have a defined rule given the large amounts of variance in how foundations report data, stratify their programs, and define their interests. However, some general patterns in the ways I produce these estimates include:
- In general, I assumed that centring on a relatively narrow set of interventions and search terms meant I was likely missing a number of interventions relevant to biosecurity. My guess is this is particularly true of various health-system strengthening interventions; lab governance, and technical research not explicitly on pathogenesis. Therefore, there were a number of cases in which I treated key terms as exhaustive of biosecurity. This is generally true of key interventions such as “vaccines” or programs focusing on “infectious diseases” that weren’t targeting neglected tropical diseases.
- Most cases involved value judgements on specific grants, which is a source of a great deal of variance. Hence, I similarly adopted quite a low bar for upper-bound figures and often a much higher bar for lower-bound figures. In many cases, this led to quite wide ranges, such as the Chan and Zuckerberg Initiative ($3.4m-$34mm).
- There were a few foundations I essentially regarded as entirely biosecurity-oriented, namely FluLab, and CEPI.
- I generally tried to keep to recent (post-2020) annual reports and grants to ensure some standardisation. Although given the large number of foundations I initially looked at (100+), this was not always possible.
- I did not distinguish between grants awarded and grants paid, as foundations tend to report one or the other. However, in many cases (especially the larger foundations), my estimates represent amounts spent on large projects. Therefore, I assume my overall estimate is closer to the spend. However, the confidence intervals are likely wider than the average difference between grants paid and grants awarded, so I was not too concerned about this.
- In my second pass, I focused more on producing higher fidelity estimates of the big players. Supplementary data for some of these estimates can be found in the spreadsheet (for example, here).
- I was also concerned about double-counting in a few cases (especially CEPI). For example, it was unclear how much of CEPI’s spending was enabled by grants from the Bill & Melinda Gates Foundation. In these cases, my lower bound assumed total double-counting, and my upper bound assumed none.
- Finally, a large category of funding ended up being pathogenesis research. I do not have a technical background in the life sciences and found it difficult to create value judgements on how relevant these are to pandemic prevention. However, I think their spillover effects are plausibly quite large. I was likely more generous in this category than my others.
- There were a fairly sizeable number of foundations that plausibly spent little to nothing per year on biosecurity. In some of these cases I did have somewhat more accurate estimates in an earlier version. However, given the overall figures were less sensitive to these, I placed them in the <$100k range and took the average as $50,000.
In light of the above, many of these estimates per organisation are likely incorrect. However, it was unclear to me that this process was introducing a particular directional bias. Therefore, I assume that many of these inaccuracies cancel out such that the aggregated sum was likely more accurate.
Overall, this allowed me to produce a lower-bound estimate of ~$780m and an upper-bound estimate of ~1.6bn for a total estimate of ~$1.2bn. This is dominated by the Wellcome Trust (~$370m), Bill and Melinda Gates Foundation (~$330m), CEPI (~$180m), and the Novo Nordisk Foundation (~$110m) - noting very high uncertainty on CEPI and Novo Nordisk in particular.
Part II: Philanthropy Breakdown by Area
For Part II, I focused on the top funders to get a rough sense of how biosecurity funding breaks down by intervention.
My overall methodology was as follows (EDIT: I note some errors in my calculations producing these results. Updated figures are in Updates & Corrections. The method is largely the same, although I now divided the weights by the number of focus areas per org and did not manually weight GCBR focus areas given no need):
- I looked through the annual reports or websites of all funders who likely donate upwards of £1m+ according to my Part I estimate in more detail.
- Identified "key areas" that their funding breaks to and note these down. Noting:
- I ended up limiting my categorisations to the search tags I produced in Part I for consistency.
- I grouped many of these into “GCBR Priority Areas”, which encompass essentially all of the "Key Areas" identified in Part I except pathogenesis research or lab biosafety. I note that my categorisation of “GCBR Priority Areas” means I assume no overlap in GCBR Priority Areas and other areas, which is definitely not the case in practice. This likely produces upper bounds of how much issues like GCBRs and biodefense get relative to other areas.
- Each area then becomes a unique count. This assumes that funders roughly spend equal amounts in their listed areas. For this reason, my bar for a "key area" is something like this is a priority area for funders.
- The counts are weighted by the total average spend calculated in 2. Biosecurity Spending by Foundation.
- For “GCBR Priority Areas”, I aggregated all EA-aligned/EA-adjacent funders with more than £1m+ in biosecurity spending a year.
- I note that given I have actual data on exactly how much EA orgs spend, which I assume is exclusively on GCBR Priority Areas, I manually adjust the weight to represent the actual amount.
- The weighted counts are converted into percentages, which I take as reflecting the overall amount spent on biosecurity.
My breakdown is in ‘Results’, where I estimate GCBR Priority Areas represent roughly 4% of the total biosecurity philanthropic spend. However, aside from how scrappy this calculation was, I note that my delineation of GCBR Priority Areas excludes large amounts of work that would plausibly interest EAs - especially infectious disease surveillance, lab biosafety, and health system readiness.
My results suggest that most of the biosecurity spend is on infectious disease surveillance, pathogenesis research, and rapid vaccines. Noting, however, that I seemed to have underestimated how much of the biosecurity spend was on antimicrobial resistance based on the sanity check below, which is also plausibly a key focus area within biosecurity more generally.
As a sanity check, I tried to get an independent estimate for AMR funding. According to this source, Antimicrobial Resistance receives roughly ~$200 - $230m a year in philanthropic funding. My estimates produce a figure of about $140m, or about 30-40% off. My best guess is this is largely from overweighing pathogenesis research (a fair amount of which is aimed at AMR). However, I think being off by less than a factor of 0.5 was pretty good for a rough calculation.
I reiterate that this is very scrappy, and only around 3 hours were spent on this estimate, so there is quite a lot of uncertainty. However, a key cause of uncertainty is the distribution of spend amongst the very big players, who don't prioritise GCBR Priority Areas. I also note my assumption that this funding is mutually exclusive produces a slight overestimate. Therefore, I would guess it is highly unlikely that philanthropic spending on technologies such as far-UVC, preventing bioterrorism, synthesis screening, and regulating dual-use research of concern represent more than 5% of the total biosecurity spend.
Part III: Biosecurity BOTECs
Finally, I initially aimed to independently sanity-check my Part I calculations via a BOTEC. This process led me to collect some additionally useful pieces of information
My overall methodology was as follows:
- I first aimed to produce estimates of how much public health philanthropy takes place overall. I note this method assumes biosecurity is a subset of public health. For the reasons I state in ‘About’ this is quite flawed. However, most biosecurity spending that is not under the public health bracket are national security interventions that currently represent a small proportion of the total biosecurity spend according to my Part II calculations. Therefore, I felt this assumption was reasonable.
- There was a lot of variance, so I used 5 different methods and produced an estimate by averaging these:
- Method 1 involved finding a source on global giving in the US; the share of total philanthropic giving in the US; what proportion of global philanthropy the US represented (~50%), and then using this to estimate total public health philanthropy.
- Method 2 involved estimating public health research spending, and then scaling this by the proportion of health research spending:health spending by the UK government. This was a very, very rough method, and is likely an overestimate as one would expect philanthropy to be overrepresented in health research spending versus object-level spending on healthcare by a lot.
- Method 3 involved finding a source on how much public health philanthropy there was in the US; what proportion of global philanthropy the US represented, and then using this to estimate total public health philanthropy.
- Method 4 involved a McKinsey source on annual health grant funding that I scaled by the proportion of global philanthropy the US represented, using this to estimate total public health philanthropy.
- Method 5 involved me just collecting two additional figures based on spending by the top 100 grantmakers and an additional source for healthcare philanthropy.
- I note many of these calculations rest on this statistic that the US represents roughly half of global philanthropy. This was roughly commensurate with another source I found noting that 61% of philanthropy dollars are US-based. However, I appreciate that this introduces wide uncertainty on all of these figures.
- There is an extremely wide variance ($46m to $300m) generally stemming from operationalisation. In particular, variance in measuring levels of philanthropy is driven by whether you're talking about donations to foundations, foundation awards, foundation fundraising, or foundation spending, as well as how you account for cashflows between foundations, governments, and charities. These estimates are deeply quite uncertain.
- However, I sanity-checked my result (~$130m) according to a figure I could find of how much of global philanthropy is spent on healthcare and figures on total philanthropic spending in 2020. My estimate came to 50% of philanthropic spending being public health, which was quite close to the 44% quoted in the Forbes article.
- To now estimate what % of public health spending is biosecurity, I produce an upper bound by anchoring on US and UK data on (i) biosecurity budgets and (ii) health budgets. I get a figure of ~1.5%.
- This figure of 1.5% is a very clear overestimate as the UK and US spend more on biosecurity than most other countries in the world. I round it down to 1%, which is probably still an overestimate, although I do note that the vast majority of most biosecurity spending seems to be from the US.
- I think this is among my shakiest assumptions, although if 1.5% is an absolute upper bound that assumes the rest of the world spends on biosecurity commensurate with the US, then given US government expenditure is roughly 33% of total government spending worldwide, this is effectively the same as suggesting the rest of the world is spending 0.75% of their public health budget on biosecurity. Looking at figures for the UK (see the spreadsheet) and Australia (from this source on their biosecurity spending given their health budget, where these amounts are ~0.5%-1.1%), this makes 0.75% plausibly still an overestimate, but more feasible than 1.5%.
- With this 1% figure, I estimate that ~$1.3bn is spent on biosecurity by philanthropy as an upper bound.
- The results of my foundation calculations were an upper bound of ~$1.6bn. This is good convergence, especially given both included some generous assumptions. In turn, I take the $1.3bn upper bound with the lower bound from the foundation list to produce more conservative average.
- In turn, I conclude that ~$1bn is spent on biosecurity a year by foundations.
- This encompasses a "loose" definition of biosecurity in which issues like influenza, COVID-19 response, Antimicrobial Resistance, strengthening rapid response, and understanding pathogenesis are included.
- Issues like malaria, tuberculosis, and broader public health concerns are not intentionally included. However, given many foundations have an "infectious diseases" program, I leant towards including these. I'd guess (low-confidence) this means my estimate could be blown up by as much as 20-30%, although it is difficult to say as many infectious diseases programs are still relevant to pandemic prevention (especially concerning technologies, laboratory capabilities, and surveillance).
- I collected some additional data to contextualize these findings. See ‘Results’ for more details.
Overall, there is an enormous degree of uncertainty. However, I do think this is likely to be accurate within a factor of 2-3. Given my line-by-line estimates in Part I, I would be surprised if I underestimated by more than $500m. Depending on how loosely one defines biosecurity, it is easy to find $500m in biosecurity funding from the annual reports of Bill & Melinda Gates and the Wellcome Trust alone. I think my risks of this being an overestimate are greater. However, I think it is difficult to find evidence of more than $3bn in philanthropic funding for biosecurity. I am fairly confident (~70%) of a range of about $500m - $2bn, with my best guess being in the $700m - $1.1bn range.
Results
Part I: Biosecurity Spending by Foundations
Overall, I arrived at a lower-bound estimate of ~$780m and an upper-bound estimate of ~1.6bn for a total estimate of ~$1.2bn using this method, noting I think it is probably an overestimate and update it in light of my later BOTECs. My breakdown of funders I estimate spend more than $1m a year on biosecurity is as follows (note that due to currency conversion precise figures may change):
Fig. 1 - Biosecurity Philanthropy by Foundation ($1m+)
| Funders | ||||
| Organisation | Total Annual Biosecurity Awards (LB) | Total Annual Biosecurity Awards (UB) | Total Annual Biosecurity Awards (Average) | Areas (£1m+) |
| £100m+ a year | ||||
| Wellcome Trust | $373,607,175.00 | $373,607,175.00 | $373,607,175.00 | Rapid Vaccines, AMR, Foundational PPR, Disease Surveillance, Therapeutics |
| Bill & Melinda Gates Foundation | $194,000,000.00 | $462,000,000.00 | $328,000,000.00 | Rapid Vaccines, Foundational PPR, Disease Surveillance, Therapeutics |
| CEPI | $27,000,000.00 | $327,000,000.00 | $177,000,000.00 | Rapid Vaccines |
| Novo Nordisk Foundation | $17,157,438.00 | $201,618,364.00 | $109,387,901.00 | Foundational PPR, AMR |
| £10m - £100m a year | ||||
| The Rockefeller Foundation | $31,676,492.33 | $45,217,341.00 | $38,446,916.67 | Disease Surveillance, Rapid Vaccines, Health System Readiness |
| FluLab | $26,142,780.89 | $36,966,268.83 | $31,554,524.86 | Disease Surveillance |
| Open Philanthropy | $30,000,000.00 | $30,000,000.00 | $30,000,000.00 | GCBR Priority Areas |
| Skoll Foundation | $20,000,000.00 | $20,000,000.00 | $20,000,000.00 | Rapid Vaccines, Therapeutics, Disease Surveillance, PPE |
| Chan Zuckerberg Initiative | $3,400,000.00 | $34,000,000.00 | $18,700,000.00 | Foundational PPR, Disease Surveillance |
| The Fondation Mérieux | $15,125,426.67 | $15,125,426.67 | $15,125,426.67 | Disease Surveillance, Laboratory Preparedness |
| Effective Giving | $10,000,000.00 | $10,000,000.00 | $10,000,000.00 | GCBR Priority Areas |
| £1m - £10m a year | ||||
| Illumina Corporate Foundation | $3,600,000.00 | $12,000,000.00 | $7,800,000.00 | Disease Surveillance |
| Burroughs Wellcome Fund | $7,320,000.00 | $7,320,000.00 | $7,320,000.00 | Foundational PPR, Fieldbuilding, DURC |
| CDC Foundation | $5,100,000.00 | $5,100,000.00 | $5,100,000.00 | Disease Surveillance, Laboratory Preparedness |
| Survival and Flourishing Fund | $1,700,000.00 | $1,700,000.00 | $1,700,000.00 | GCBR Priority Areas |
| W. M. Keck Foundation | $1,000,000.00 | $2,333,333.33 | $1,666,666.67 | Foundational PPR, COVID-19 |
| Musk Foundation | $1,333,333.33 | $1,333,333.33 | $1,333,333.33 | AI-Bio |
| Founders Pledge | $1,000,000.00 | $1,000,000.00 | $1,000,000.00 | GCBR Priority Areas |
I note again that many of these estimates per organisation are likely incorrect, but I do think the aggregate sum is more likely accurate. I would not place tons of stock in the exact figures.
See the full results here.
Part II: Philanthropy Breakdown by Area
My rough breakdown of biosecurity spending by area is as follows (EDIT: I note some errors in my calculations producing these results. Updated figures are in Updates & Corrections).
Fig. 2 - Biosecurity Philanthropy by Area
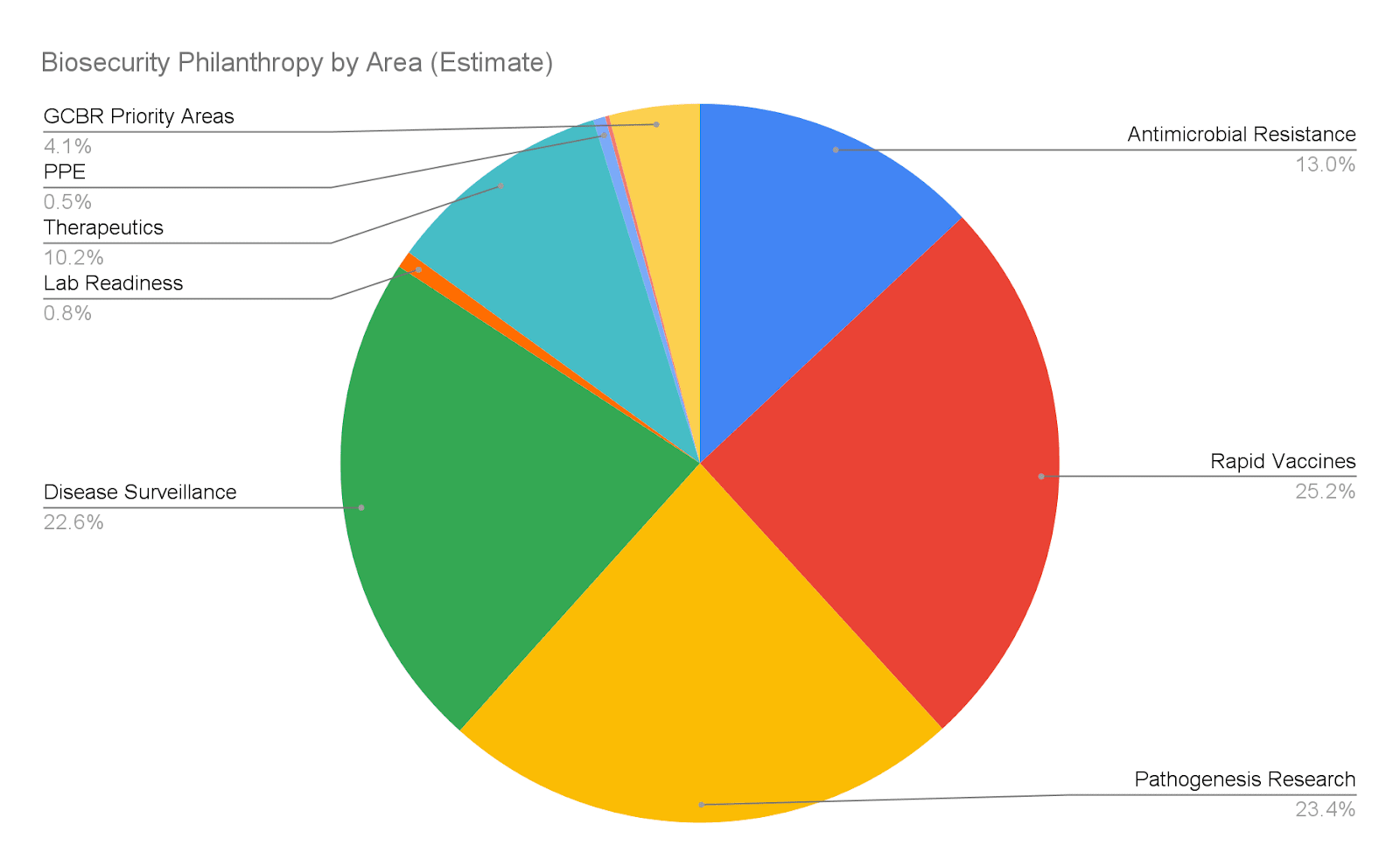
My actual estimates are as follows:
Fig. 3 - Biosecurity Philanthropy by Area Table
| Area | Weighted $ |
| Antimicrobial Resistance | $134,767,113 |
| Rapid Vaccines | $261,169,371 |
| Pathogenesis Research | $242,580,804 |
| Disease Surveillance | $233,751,234 |
| Lab Readiness | $7,900,141 |
| Therapeutics | $105,954,834 |
| PPE | $5,576,570 |
| DURC | $1,858,857 |
| GCBR Priority Areas | $42,288,991 |
See the full results here.
Part III: Biosecurity BOTECs
The most relevant statistics are the following:
- I estimate that public health spending breaks down into:
- $9.8tn in total is spent on public health.
- $7.7tn of this is spent by governments (~79%).
- $130bn of this is spent by foundations (~1.3%).
- The remainder likely comes from private spending and public-private partnerships that aren't independent foundations (e.g. universities).
- I estimate that biosecurity spending breaks down into:
- $1bn by foundations.
- Assuming that the ratio of biosecurity to public health for governments is roughly 1%, ~$100bn is spent by governments on biosecurity. However, I think this is very plausibly a large overestimate (e.g. by a factor of ~2).
- As a sanity check, the Biological Weapons Convention has a budget of around $1.8m a year and the much larger Global Partnership Against the Spread of Weapons and Materials of Mass Destruction spent roughly $2bn across 25 members in 2023.
- Assuming the ratio of government spending to total spending is 1:1.27 (given public health spending), then ~$130bn is spent on biosecurity globally.
- Some further implications:
- Biosecurity philanthropy is ~0.8% of public health philanthropy and ~1% of what governments spend on philanthropy.
- The US biodefense budget was approximately $24.3bn in 2023, making the US government a considerable funder of biosecurity globally.
- Where EA fits in:
- EA players represent ~4% of the total biosecurity spend.
- EAs are also interested in infectious disease surveillance, vaccine development, antimicrobial resistance, and developing broad-spectrum antivirals. However, EAs are likely not the majority in these spaces.
- My own impression (quite low-confidence!) is that spending on EA focus areas like technologies such as far-UVC, synthesis screening, and GCBR-specific concerns is likely dominated by EA. Spending on preventing bioterrorism, bioweapons, and policy advocacy with respect to biosecurity is also likely majority EA (but not necessarily exclusive).
See the full results here.
Takeaways
What can we conclude about biosecurity philanthropy and the biosecurity funding landscape from this? I would generally caution not too much. As stated in ‘Why Does This Matter, I would caution against assuming that far-UVC interventions are substantially more neglected than early-detection interventions. I think such an assessment would require priors about the probability distribution of threat models, pathogen characteristics of concern, pandemic intensities, and all manner of practical considerations - but also far more detailed knowledge about how money is being spent in these areas than I have presented here.
I should also note that this is a loose, generally post-COVID, snapshot that poorly generalises to the past and likely does not predict the future. Many of these organisations expanded their biosecurity funding post-COVID and projects like CEPI were founded. However, we should not assume that this status quo is at all fixed.
However, I do think the rough and order-of-magnitude estimates at least provided me with a number of useful and potentially decision-relevant insights. These are some of my thoughts:
- Biosecurity philanthropy is probably a relatively small part of total biosecurity efforts, with the US government probably being the largest player.
- Biosecurity is a relatively small part of public health, both in philanthropy and government spending. While I have arbitrarily delineated between the two, however, I reiterate that many public health interventions are in practice targeting the same goals and may be relevant for mitigating GCBRs. I’m cautious that the assumption that global health is saturated risks neglecting opportunities to mitigate GCBRs through interventions that may be able to attract substantially more capital.
- The biggest funders in biosecurity are the Wellcome Trust, Bill and Melinda Gates Foundation, CEPI, and the Novo Nordisk Foundation. Accounting for uncertainty, Open Philanthropy is probably the fourth to eighth biggest funder of what I’ve considered ‘biosecurity’. I think it’s important for many to realise the importance of other players and funding sources in the landscape. This could mean many more funding opportunities EAs are systematically neglecting.
- However, and though this view is even lower-confidence, I was struck by how little philanthropy has been directed towards tech development for biosecurity, mitigating GCBRs, and policy advocacy for a range of topics from regulating dual-use research of concern (DURC) to mitigating risks from bioweapons. I do think this may suggest some leveraged opportunities for funders and organisations to contribute a great deal.
- Most biosecurity funding and philanthropy are US-based, although I note the Wellcome Trust is UK-based. My impression is there is very little money focusing on biosecurity in LMIC contexts, even though they will increasingly represent a larger share of GCBRs. Taking Africa, for example, I note last year’s break-in to a BSL-3 lab in Sudan, South Africa’s former history of developing bioweapons, and a rise in zoonotic transmission from Africa.
However, for some of the reasons I’ve stated, I remain cautious about making inferences about what the absolute amount of money means in biosecurity, the relative neglectedness of interventions, and how well EA concerns about biosecurity are represented in biosecurity more generally. I think we’re quite a while away from being able to conduct rigorous, all-in, cost-effectiveness analyses of the benefits of different interventions. However, I’m also not sure it’s necessary to make progress on biosecurity.
The biosecurity field is filled with a number of technologies, strategies, and interventions that seem robustly good and will likely be neglected given the sheer heterogeneity of threat scenarios one could construct; contexts these threat scenarios could emerge in, and contingencies that affect the successes of various interventions. Many of these do not obviously rade off against each other and the vicissitudes of policy mean that we should expect policy windows to help drive our prioritisation.
However, I do think that considering the funding landscape can be useful for helping to better calibrate the state of play; identify what uniquely leveraged opportunities to contribute towards biosecurity might look like, and demonstrate just how much more we could be doing to ensure that the world is adequately protected from pandemics of all severities.
Next Steps?
I think dozens of hours could be sunk into producing a higher-quality version of this that might be more decision-relevant for funders and organisations in biosecurity. However, I think this would have to be one of many research pieces required to be able to do effective, all-things-considered, assessments on what problems to work on in biosecurity and what interventions are the most promising. Updating this or making it more rigorous is not currently a priority of mine, although I do intend at least for the next few months to incorporate feedback into my estimate and to correct any grave errors. Any and all feedback would be exceptionally welcome!
If you’re interested in taking this further in any capacity, please reach out to me directly, and I’d be happy to discuss next steps.
Updates & Corrections
[05/04/2024]
Many thanks to @Angelina Li for catching an error in my calculation of philanthropy by area: I forgot to divide the total weight per org by the number of focus areas they have. I'm also very grateful for Angelina's revisions which I've added to the calculations. I note the updated estimates below, though they are not drastically different from my original estimates (all most likely within the 95% confidence interval given high levels of uncertainty).
Fig. 2 - Biosecurity Philanthropy by Area
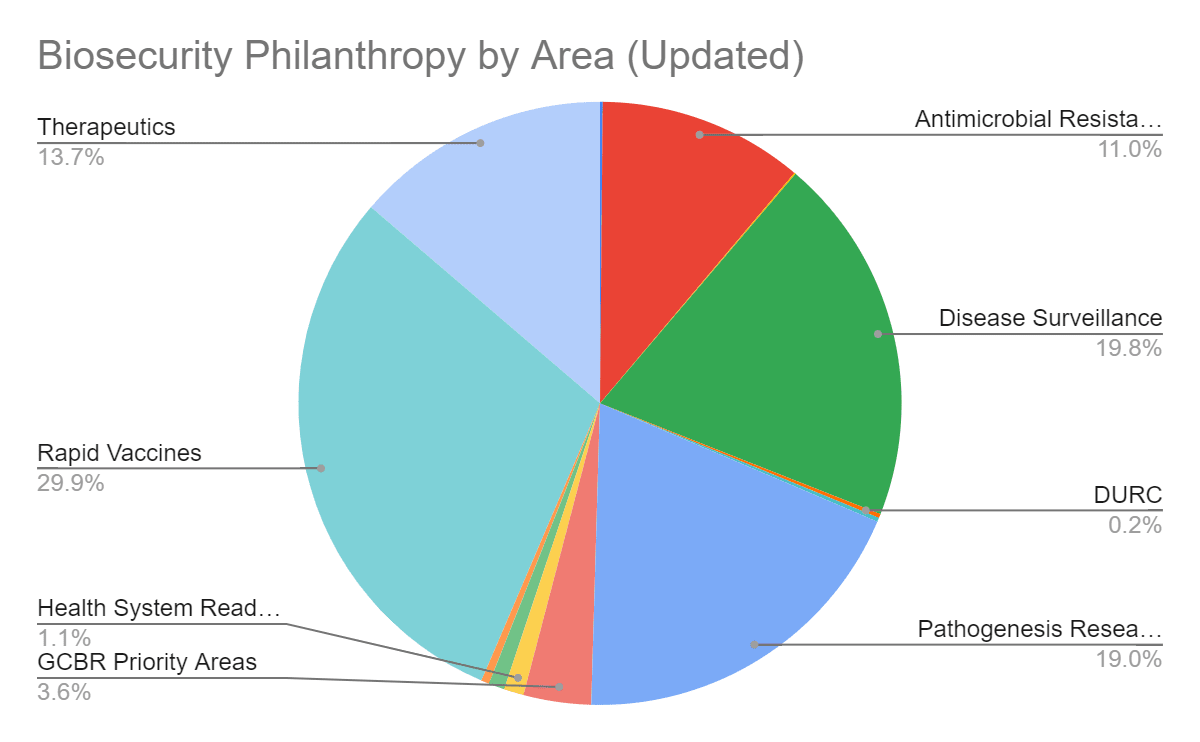
The updated table is here:
Fig. 3 - Biosecurity Philanthropy by Area Table
| Area | Weighted $ |
|---|---|
| AI-Bio | $1,472,633 |
| AMR | $114,129,071 |
| COVID-19 | $736,317 |
| Disease Surveillance | $204,696,010 |
| DURC | $2,208,950 |
| Fieldbuilding | $2,208,950 |
| Pathogenesis Research | $197,332,845 |
| GCBR Priority Areas | $37,552,146 |
| Health System Readiness | $11,044,749 |
| Laboratory Preparedness | $8,835,799 |
| PPE | $4,417,900 |
| Rapid Vaccines | $309,252,965 |
| Therapeutics | $142,109,101 |
Also made changes to acknowledgements.
[23/04/2024]
Many thanks to @EU Policy Careers for flagging my misunderstanding of this source which led me to conclude the US government spends ~$88bn on biosecurity. The actual answer, per CSR's estimates, was ~$24.3bn in 2023. I've corrected this in the article, and additionally make two notes:
- My estimate of ~$100bn being spent by governments on biosecurity was due to the assumption that the ratio of biosecurity to public health for governments is roughly 1%. But this anchors on the incorrect US statistic I used earlier and the figures for the UK. I note I rounded down from a US-UK average of 1.5% anyway, but this makes me more confident that this ratio is still an overestimate. I think $100bn is effectively an upper bound, and it could feasibly be half (if not more) this. I've tried to reflect this in the main passage of the text. I no longer have a good estimate of what % of the total biosecurity government spend the US constitutes. I've tried to reflect these updates in the main text.
- This formerly led me to conclude that "the clearest way to shift large amounts of money towards biosecurity would be via US policy". I still suspect this is true, but I am considerably less confident. I've removed it from the main text.
This is interesting, thanks for sharing! :)
I was browsing your BOTEC and wonder if I've found a bug or two in sheet 3 (but it's possible I'm not understanding something about your methodology, I only took a quick look / haven't read this post in detail).
On sheet 3, I think the weights are meant to basically represent how much money is being spent in each org + category, relative to the smallest org you look at? (W. M. Keck Foundation).
But it looks like you're not dividing the total weight per org by the number of focus areas that org has. So i.e. here I think here the weights for Wellcome > AMR should be =round(223.45 / 5), since you list 5 focus areas for Wellcome on sheet 1. I might be misunderstanding something here (only took a cursory check).
Also it looks like you're missing the Therapeutics category for Wellcome + Lab Readiness for Rockefeller, I think? (Maybe some others too).
I tried fixing this by making some changes (highlighted in green) here, mostly in sheet 3 (starting col L) and a bit in sheet 1. Happy to give you edit access if you request it.
Also sorry if this is too nitpicky, I just like auditing spreadsheets :) Thanks for publishing this!
Really appreciate you picking this up! Edit access would be great - I've sent a request and will then incorporate the necessary fixes.
Granted :)
I think you made a mistake in calculating summary statistic #3, claiming that the US government makes up the bulk of government biosecurity spending globally. Using a yearly rather than the 5-yearly figure you seem to use for US government spending, the US share in global biosecurity government spending seems closer to 25% rather than the 90% you suggest.
It seems that you used the $88.2bn figure from this White House source you quote below as an estimate for the US government annual biosecurity budget. However, the source explains that the $88.2 billion is a 'request for mandatory funding available over five years', not annually. Further, this is only the requested budget by the Biden administration, not the final spending figure. Not exactly sure on this, but the actual levels of funding are (likely?) to be (significantly?) lower after the budget passes Congress.
A better figure would be the estimates by the Council on Strategic Risks on biosecurity spending in past years - e.g. $23bn for 2023 (which also include DoD spending in addition to HHS, NIH, ASPR, FDA, USAID and CDC from the White House Source).
Taking your very rough estimate of $100bn global annual government spending on biosecurity as given, this would result in the US only making up ca. 25% of global biosecurity government spending rather than 90%. Intuitively, the 25% figure perhaps underestimates the role of the US government - perhaps as the $100bn global sum seems a bit high, but low confidence on both of those statements, further research here would be very interesting.
However, correcting the 90% figure downwards seems like an important correction to the piece and its conclusions, as the GCBR policy community is arguably already disproportionately focused on the US/UK, with biosecurity policy in other parts of the world still neglected.
Thank you so much for flagging this! Very much agreed this is an important correction; the update that the US doesn't dominate the biosecurity spend this way is indeed important and I think a welcome one. Will certainly amend.
Interesting work, and some smart/decisive decision-making in terms of methodology. There is a trade-off in the effort required to map and data mine funding streams exhaustively, and what you have done makes a lot of sense.
Have you considered spot comparisons of the data included here against existing R&D funding repositories like Policy Cures Research's G-FINDER or NIH World RePORT? (disclosure that I used to work at PCR). For purely product-related R&D expenditure, I think, it supports your approach in that there are only a few funders not already identified in your dataset (Fundació La Caixa and Michael & Susan Dell Foundation of note). I do think there is less meaning in trying to reconcile funding estimates, and more important in identifying the relationships and approximate/relative quantum of funding.
An additional lens of analysis would be to try to map philanthropic biosecurity recipients and sources/magnitude of funding towards these organizations - illustrating to potential funders where resources might be allocated in the philanthropic biosecurity space.
This is great, thank you for doing this hard work!
A couple of disagreements:
"I think it’s important for many to realise the importance of other players and funding sources in the landscape. This could mean many more funding opportunities EAs are systematically neglecting."
My view is that many players and funding sources means that fewer important funding opportunities will be missed.
"I was struck by how little philanthropy has been directed towards tech development for biosecurity, mitigating GCBRs, and policy advocacy for a range of topics from regulating dual-use research of concern (DURC) to mitigating risks from bioweapons."
I 100% agree regarding policy advocacy, but I disagree regarding tech development and mitigating GCBRs for reasons you do mention - that many different interventions, including vaccine R&D and broad public health systems strengthening in LMICs, contribute to mitigating GCBRs.
Appreciate the kind words!
I think I'd push back somewhat although my wording was definitely sloppy.
I think it's worth establishing my frame here because I reckon I'm not taking neglectedness in a more conventional sense along the lines of "how much biorisk reduction is on the plate?". I generally think it's quite hard to make judgements about neglectedness in this way in bio for two main reasons: firstly, many interventions in bio are only applicable to a particular subset of threat models and pathogen characteristics and can be hugely sensitive to geographic/local context amongst other contingencies. Secondly, there are no great models (I could find!) of the distribution of threats by threat models and pathogen characteristics. So when I'm talking about neglectedness, I think I mean something more like "how many plausible combinations of threat models, pathogen characteristics, and other contingencies are being missed".
"My view is that many players and funding sources means that fewer important funding opportunities will be missed"
So I think this could turn out to be right empirically, but it's not trivially true in this instance if most funders centre on a narrow subset (e.g. naturally emergent pandemics; respiratory transmission; flu-like illness); EAs focus on quite specific scenarios (e.g. genetically-engineered pandemics; respiratory transmission; high case-fatality rates), but then this leaves a number of possibilities that could contribute towards reducing threats from GCBRs that other funders could be interested in. For example, smallpox; antimicrobial resistant strains of various diseases; or even genetically-engineered diseases that might not directly be GCBRs. I think a key assumption here is that work on these can be doubly relevant or have spillover effects even for models that are more GCBR-specific. Hence why, I conclude that many opportunities "could" be missed: the failure mode looks like a bioinformatics company working on the attribution of genetically engineered pathogens and neglecting funding from the much more well-funded antimicrobial resistance landscape, even if there's a lot of overlap in methods and the extra resources could drive forward work on both.
"I was struck by how little philanthropy has been directed towards tech development for biosecurity, mitigating GCBRs, and policy advocacy for a range of topics from regulating dual-use research of concern (DURC) to mitigating risks from bioweapons."
This is definitely poor wording, poor grammar, and an important omission on my part, haha. What I want to stress though is "tech development for a range of topics" / "mitigating GCBRs for a range of topics", and by "for a range of topics" I want to refer to a particular subset of misuse-based concerns that vaccine R&D, health system readiness, and pathogenesis research are less applicable to. A naive example of this would just be "wildfire" cases with unforeseen transmissibility and case fatality such that countermeasures or general health systems strengthening would probably be less effective here than focusing on prevention.
My surprise ultimately comes from the fact that I think both in EA and outside EA - admittedly noting I don't have lots of experience in either - people do internalise the sheer heterogeneity here. I don't think levels of funding/concern have ever really well-tracked what threats we should be most concerned about. But in turn, I guess I was taken aback to still see these gaps (and hopefully opportunities!) on both ends.
Executive summary: An analysis of biosecurity philanthropy funding estimates that approximately $1 billion is spent annually, with most funding coming from a few large foundations and focused on areas like infectious disease surveillance, pathogenesis research, and vaccine development rather than existential risk priorities.
Key points:
This comment was auto-generated by the EA Forum Team. Feel free to point out issues with this summary by replying to the comment, and contact us if you have feedback.
Thanks for sharing, Conrad!
I wonder whether Open Philanthropy (OP) should have commisioned an analysis like yours much sooner. More importantly, I am a little confused about why OP would want to know how much is being spent on biosecurity & pandemic preparedness at this stage. Neglectedness may be a good heuristic to identify promising areas at an early stage, but OP has now granted 191 M$ to interventions in that area, according to their grants' database on 17 February 2024. So I would have expected OP to be focussing on the marginal cost-effectiveness of their grants. In addition, I think this should be assessed not only in terms of reducing tail risk, but also in DALY/$, as it is typically the case for public health interventions.
I have been recently asking around whether someone has compiled how much money is going into different ways of mitigating GCBRs, so this is quite relevant! Do you have estimates of the current EA (or otherwise) spending in these or similar buckets?
Yeah, great question! Lots of these categories were things I thought but ultimately had difficulties getting good estimates, so I don't have good answers here. But I can say a little bit more about what my impressions were for each.
1. AI-misuse is tough because I think lots of the work here is bucketed (usually implicitly) into AI safety spending which I wasn't looking at. Although I will say I struggled to find work at least explicitly focused on AI-bio that wasn't EA (usually OP) funded (e.g. RAND, CLTR). I think in turn, I capture a lot of this in my "GCBR Priority Areas" bucket. So at least as far as work that identifies as attempting to tackle this problem it's some % of this bucket (i.e. probably in the $1m-$10m order of magnitude, could be a fair bit less), but I don't think this reflects how much total is going towards biorisk from AI, which is much harder to get data on.
2. Yeah synthesis screening I definitely implicitly bucket into my "GCBR Priority Areas" category. I didn't attempt to break these down further because it'd be so much more work, though here's some thoughts:
Synthesis screening is hard to get data on because I couldn't find out how the International Gene Synthesis Consortium is funded, and I think historically this represents most of the biosecurity and pandemic prevention work here. My best guess (but like barely more than 50% confidence) is that the firms who form it directly bear the costs. If true, then the work I could find outside this space that is philanthropically funded is NTI | bio / IBBIS and SecureDNA/MIT Media Lab. NTI spent ~$4.8m on their bio programs and has received OP funding. MIT Media Lab have received a number of OP grants, and SecureDNA list OP as their only philanthropic collaborator. This means the spend per year is probably in the $1m-$10m order of magnitude, most of which comes from EA. Though yes the IGSC remains a big uncertainty of mine.
2. I think breaking down disease surveillance into pathogen-agnostic early detection, 'broad-spectrum', pathogen-specific, and GCBR-specific work is pretty tough, mostly because lots of the funded work is the same across these (e.g. improving epidemiological modelling capabilities; improving bioinformatics databases; developing sequencing technology) - and there is a lot of work on all of the above. Certainly, when it comes to funders or projects identifying as being focused on GCBRs (including the 'stealth' vs ' wildfire' terminology), I could not find anything that wasn't affiliated with EA at all, which places an upper-bound at like 4-5% of the early detection spend. But for the reasons I've stated I think this is a very poor estimate of how much money actually contributes towards GCBRs and have no good numbers.
3. Outside of government funding/government-funded sources like univerisites, I could find no non-EA funding on P4E/resilience work. My impression is that EA represents most of the far-UVC work and thinking about pandemic-proof PPE (given that there's quite clearly attributable work to EA-aligned/EA-funded orgs like SecureBio, Gryphon, and Amodo and little work outside). But I think this is much shakier when it comes to resilience and backup plans, which would come under a lot more general resilience work. That I'm just way less sure.
4. Medical countermeasures are very similar to disease surveillance - the "therapeutics" category ideally captures these (including the development of platform technologies at places like CEPI), but delineating between GCBR-oriented countermeasures was both pretty difficult and, I think, effectively unhelpful. Lots of pathogen-agnostic work here isn't even done for pandemic-related reasons (e.g. building tools against neglected tropical diseases). Work that identifies as being focused on GCBRs, however, is essentially EA. So, whilst I think we can apply the same heuristic as for GCBR-specific early detection (at most 4-5% of the funding here), I'd be even less confident about these estimates representing the actual contribution towards GCBRs.
Hopefully this is useful!
Thanks for doing this! You say "My own impression (quite low-confidence!) is that spending on EA focus areas like technologies such as far-UVC, synthesis screening, and GCBR-specific concerns is likely dominated by EA" and I'm trying to figure out precisely how dominant EA is.
You say "Therefore, I would guess it is highly unlikely that philanthropic spending on technologies such as far-UVC, preventing bioterrorism, synthesis screening, and regulating dual-use research of concern represent more than 5% of the total biosecurity spend." And also EA funding is ~4% of total biosecurity spend. Can we conclude from this that EA is likely >80% of GCBR-specific funding?
I'm not hugely confident, but yes >80% of GCBR-specific funding from within philanthropy being from EA seems right to me.
It's generally quite hard to find GCBR-specific work outside EA that aren't from policy institutions such as Nuclear Threat Initiative, the Bipartisan Commission for Biodefense, or the Centre for Health Security - all of whom, as far as I can tell, are recipients of Open Philanthropy funds. Other work here just seem much more EA-aligned (e.g. CSER, CLTR, FLI).
Additionally, it seems likely that even insofar as these institutions care about GCBRs, EA (particularly Open Philanthropy) has been at least somewhat influential in driving this. Certainly, of the foundations that fund the Centre for Health Security, Open Philanthropy is the only one with an express mandate for GCBRs. Only Bill & Melinda Gates and Rockefeller Foundations are larger foundations than OP here, noting though I couldn't find much evidence of Bill and Melinda Gates money directly going towards CHS, and the Rockefeller funding I could find was on supporting work on the COVID-19 response. Most of the other foundations are just smaller. The Bipartisan Commission for Biodefense's most GCBR-relevant work (particularly the Apollo Program for Biodefense and other work in 2021) was produced around the same time they received a series of grants from Open Philanthropy.
I'd imagine most GCBR-specific funding probably comes from the government (the US government in particular). But yes, as far as I can tell, EA probably represents 80+% of philanthropic funding towards GCBRs.
Thanks for writing this up! Have you spoken to Christian Ruhl or anyone else at Founder's Pledge about this work? I think FP would be interested in and benefit from this.
Thank you! Yes I've been in touch with Christian Ruhl :)