TLDR: GOAL 3’s IMPALA patient monitoring system has shown extremely promising results, with initial cost-effectiveness estimates ranging from $1.61 to $3.35 per life-year saved. This is based on a 42% reduction in pediatric mortality in a Malawian hospital over 18 months and a 27% reduction in neonatal mortality in a Tanzania hospital over 12 months. Supported by a $260,000 grant from Founders Pledge and its community, we are now conducting studies to further assess While these results are encouraging, we seek feedback from the community to ensure the robustness of our methodology and to explore what is needed for broader support
Epistemic status: Experienced but open to further validation.
"As a medical doctor with 14 years of global health experience and five years working on the IMPALA solution, I am confident in the real-world results we’ve seen so far. However, I recognize that our current data, while promising, is still developing, and further research and input from the community are essential to confirm and strengthen these findings while balancing it against the urgency of the problem."
Dear EA Forum Members,
We need your crowd wisdom to help us evaluate our IMPALA solution. Our initial results are incredibly positive compared to existing interventions, but we want to ensure we haven’t overlooked key factors or introduced biases in our methodology.
Here’s where we’d love your feedback:
- Are our reasoning and methods sound? Have we missed any major issues or biases?
- How does our current evidence resonate with you? What else would be needed to gain your trust and the larger community?
- (How) should we highlight less obvious benefits, such as reducing workloads and societal impacts?
- How can we best engage the EA community to accelerate our mission?
After five years of hard work, I may be biased, but we’re results-driven and eager to learn. Please share your thoughts and feedback to help us take IMPALA to the next level.
Part 1: Why GOAL 3
In 2015, I worked as a tropical doctor in Tanzania and had an experience that changed my life. A premature boy was named after me (Niek) after I helped him survive sepsis and asphyxia. It was a fantastic experience that became even more special when I saw how this small Niek played with my one-year-old son, Guus, two years later.
Unfortunately, I also saw many children who were not as lucky. Treatment was available, but we could not recognize and treat the condition in time due to permanent staff shortages and a lack of adequate equipment. These deaths were unnecessary, which was the reason for starting GOAL 3: a social enterprise aiming to create a scalable, sustainable solution to help achieve more with scarce resources.
Part 2: Theory of change: facilitating a sustainable transition from reactive to proactive care.
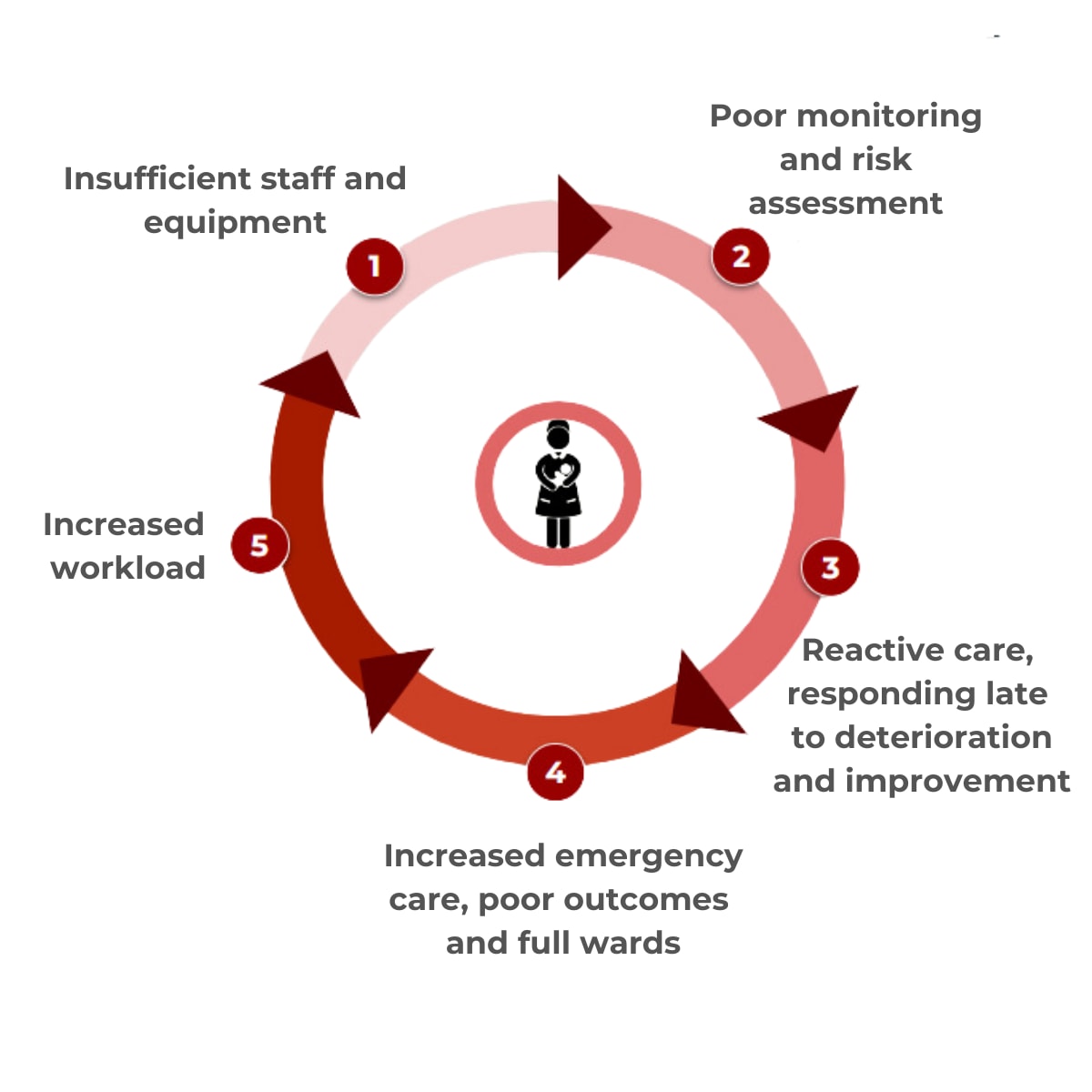
In many low-resource healthcare settings, reactive care dominates, resulting from severe understaffing and a lack of appropriate medical technology and/or information systems. Health systems typically respond to crises and acute conditions only after they’ve worsened, leading to late-stage interventions that are more costly and complex and often result in poor outcomes. This creates a vicious cycle: health workers are overwhelmed by emergencies, making it challenging to allocate time and resources for proactive care. The strain on the system leads to inefficiencies, higher costs, and worsening health outcomes—a cycle that’s hard to break due to limited resources.
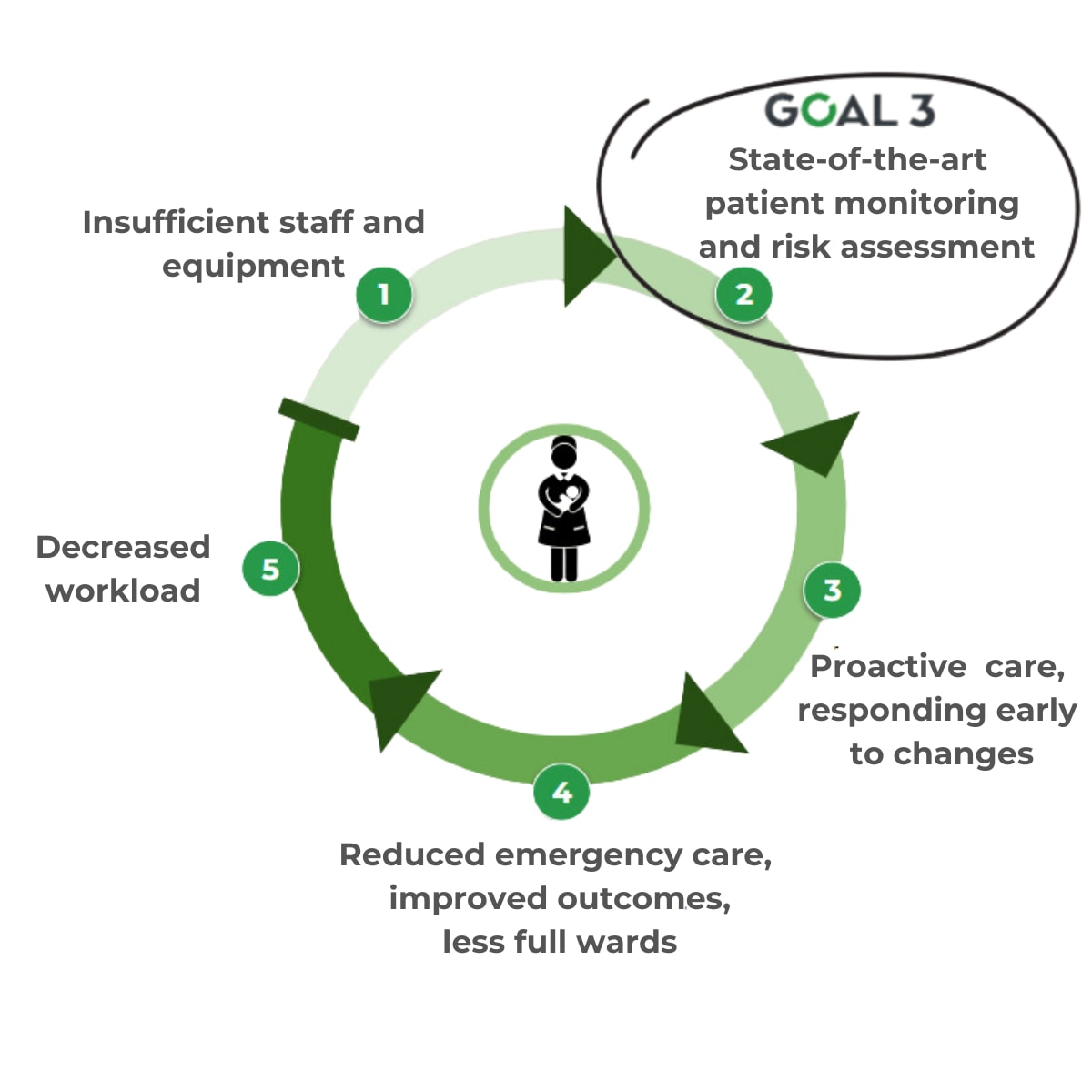
IMPALA is a patient monitoring solution that continuously measures vital signs and brings this information together in an intuitive tablet application, enabling a shift from reactive to proactive care. Through real-time data collection, intuitive risk assessment, and alarms that signal deterioration, health workers can perform timely interventions, preventing crises before they happen and reducing the need for emergency interventions.
This shift reduces healthcare providers' workloads, as fewer emergencies mean less time spent on complex, high-stress cases. IMPALA also automates routine tasks and streamlines workflows, allowing health workers to focus on direct patient care. With shorter hospital stays and fewer severe cases, the overall workload decreases, and patient and health facility costs decrease.
By breaking the reactive care cycle, IMPALA improves patient outcomes, lowers costs, and reduces the strain on healthcare workers. It is a pragmatic, scalable solution that helps health systems do more with limited resources, aligning with GOAL 3’s mission to work smarter and achieve better results.


IMPALA MonitorIMPALA Tablet
Part 3: Results from 2 pilots over 12 and 18 months: Can this really be true?
After multiple studies with IMPALA, the Ministry of Health of Malawi authorized GOAL 3 to implement IMPALA outside a research setting. In early 2023, the system was installed in the pediatric and neonatal wards in St Luke’s Hospital in collaboration with AMREF Malawi (the largest Africa-based NGO). A second pilot, involving local governments, started in Sengerema Hospital in Tanzania in July 2023, together with the Ifakara Health Institute.
The implementation of the IMPALA System involved a comprehensive approach. After an initial assessment of each facility, a tailor-made 1-day training on the use of the system and emergency and critical care was provided to all nurses, doctors, and ward attendants. After this, the system was installed in the neonatal and pediatric wards. Using a before-and-after approach, the impact on mortality and admission time of the system was monitored over time using aggregated routine patient outcome data, stored monitor data, and regular supervisory visits.
Impact on mortality
In St. Luke’s Hospital, the implementation of the IMPALA System led to a 42% relative reduction in mortality over 18 months (Feb ‘23 - Aug ’24), decreasing from 3.3% to 1.9% (p < 0.05) with 1146 admissions in the 12 months before and 1828 admissions in the 18 months after implementation. The data from the neonatal care setting could not be compared between the two periods because there was a significant change in the population due to a concurrent intervention.
In Sengerema Hospital the 12 months after implementation (Jul ’23 -Jun ‘24), neonatal mortality decreased by 27%, from 12.7% to 9.3% (p < 0.05) compared to the 12 months prior to implementation (Jul ’22 - Jun ‘23). This mortality reduction occurred while both patient admissions and in-referrals of babies born outside the hospital somewhat increased in the post-IMPALA period. This indicates that a larger and potentially more severely ill patient group was served, and therefore, the observed mortality reduction may be considered a conservative estimate of effect.
Part 4: Cost-effectiveness estimates
Pediatric care setting
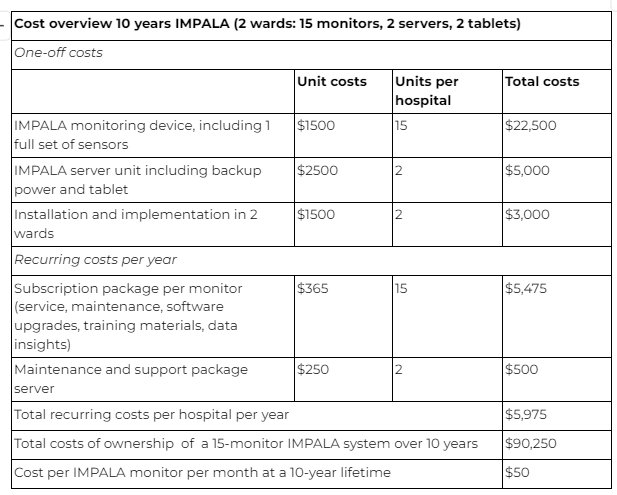
In St. Luke’s Hospital, 6 monitors were implemented in the pediatric ward for 18 months. Using the monthly total cost of ownership price of $50$, the total costs for this period were $5,400.
A total of 1829 patients were admitted during this period, and with 42% fewer deaths (1.40% absolute reduction), an estimated 26 pediatric deaths were prevented during the post-implementation period. Therefore, the cost of saving one life was $208 or $3.35 per life-year (assuming a remaining life expectancy of 62 years).
Neonatal care setting
In Sengerema Hospital, 9 monitors were implemented for 12 months. Using the total monthly cost of ownership of $50$, the total costs in this period were $5.400.
A total of 1519 patients were admitted during this period, and with 27% fewer deaths (3.38% absolute reduction), an estimated 51 neonatal deaths were prevented during the post-implementation period. The cost of saving one life was, therefore, $105 per averted death, or $1.61 per life-year (assuming a remaining life expectancy of 65 years).
In comparison to other standard-of-care interventions for preventable pediatric deaths, such as facility-based management of pneumonia (3.5$ per life-year saved), Vitamin-A suppletion (7.1$ per life-year saved), or kangaroo mother care ($20.1 per life-year saved), this initial assessment shows great potential for cost-effective impact at scale. This does not yet take into account other observed benefits, such as a reduced workload and admission time, which could translate into cost-savings for the patient and health system.
Part 5: In God we trust; all others must bring data.
But how much do we need?
While the evidence so far is extremely promising, we acknowledge its limitations. Our methodology could be improved with more direct comparisons, and we haven't yet had the resources to dive into individual-level data. Thanks to the support of Founders Pledge, we’ve launched two new studies in Malawi and Rwanda that aim to address these gaps. These studies will assess the impact on health workers, track usage data from IMPALA, and measure long-term effects on costs, outcomes, and cost-effectiveness.
Balancing Data with Urgency
We know how crucial it is to ensure IMPALA consistently delivers results across different settings. If we fail to reduce workloads or mortality, not only will we have failed in our mission, but we’ll also have spilled precious resources. That's why we are committed to being data-driven, constantly learning, adapting, and improving—because success isn’t just about if it works, but how to make it work effectively. This will be different in different settings, so implementation and evaluation are the backbone of our solution.
At the same time, I often feel frustrated by the lack of urgency. I believe we’ve found a revolutionary solution that could have a massive global impact, yet we’re still waiting for more data. When is it sufficient to take the next leap? While we focus on the costs of failure, we must also consider the cost of maintaining the status quo.
I would be delighted to hear some of your reflections on determining the right balance and what additional steps we could or should take.
What do you think?
For those who are interested, we included the link to the Cost-effectiveness assessment - a detailed analysis providing more background to our current assessment
FAQs
1.Where can I find out more about the calculation of cost-effectiveness?
- Here is a link to our website where you can download the info on our calculations: https://www.goal3.org/impact
2. Can I learn more about the IMPALA System itself?
- Sure, you can also download our product brochure from our website: https://www.goal3.org/product
- Here is also a link to our product video summarizing it shortly: https://youtu.be/fCkONDpQ8b8
3. How can I contribute to the GOAL 3 organization?
- We are always eager to hear from talented people who want to contribute. Reach out to us via the About page on our website, or consider becoming a supporter of a hospital through our GOAL 3 Foundation.
- https://www.goal3.org/about

Hi Ian, thank you for your thoughtful feedback. We fully agree that independent evaluations and randomized controlled trials (RCTs) are an important tools for understanding impact. However, we must also acknowledge that RCTs come with significant costs, long timelines, and often produce results that don’t fully translate into real-world settings. Our experience has shown that the complexity of low-resource healthcare environments requires adaptable, on-the-ground solutions that are continuously tested and refined in real-time.
That’s why, at GOAL 3, continu... (read more)