The 2023 EA Mental Health & Productivity Survey was designed to build upon the results of the 2018 and 2021 EA Mental Health Surveys, which measured the prevalence and effects of mental health problems within the Effective Altruism (EA) community and obtains more information about the experiences of community members who struggle with mental health problems, respectively. Its goal is to provide more insight into community members’ mental health and productivity issues and experiences, and to get a better idea of what resources and services people might find helpful when dealing with or for preventing these. This survey was intended for anyone wishing to improve or maintain good mental health and / or productivity, and therefore was not restricted to only those members of the community who are struggling with mental health.
This results post starts out with the demographics of the survey participants, and then covers the following topics:
- Mental Health Topics and Disorders. A more granular view of the mental health disorders and conditions or topics Effective Altruism community members struggle with or would like to improve than has previously been measured.
- State of Your Mental Well-Being. Gauging satisfaction with one's life, relationships, community, and productivity.
- Experience with Interventions. Collecting information on the types of mental health interventions people have tried, including substances.
- Demand for Interventions. Gauging interest in learning more about interventions to improve one's mental health, well-being, and productivity, and collecting information about what types of interventions people are interested in.
- Important Factors for Intervention Use Decisions. Collecting information on factors that could play a role in how people decide which interventions to use.
Demographics
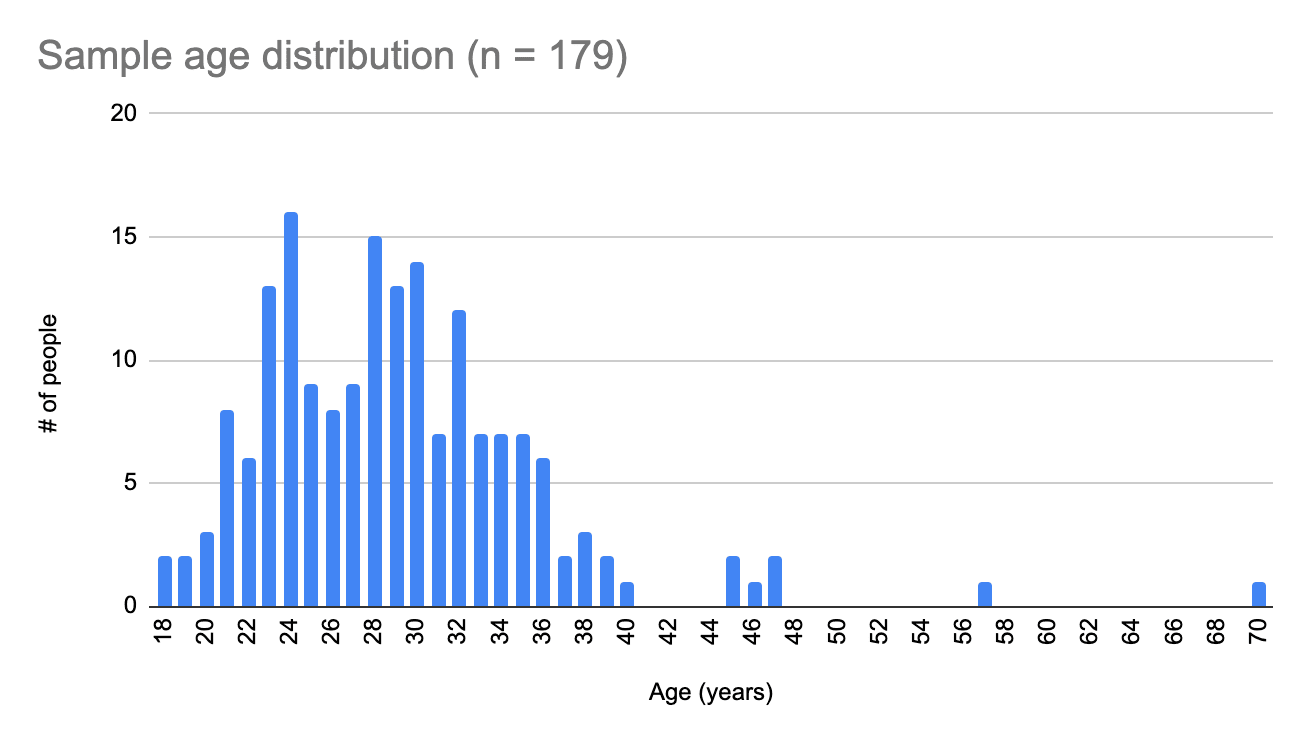
(1) Age
Ages of survey participants ranged between 18 and 70 (x̄=29.1, SD=6.8), with the majority of people in either their early to mid-twenties or late twenties and early thirties.
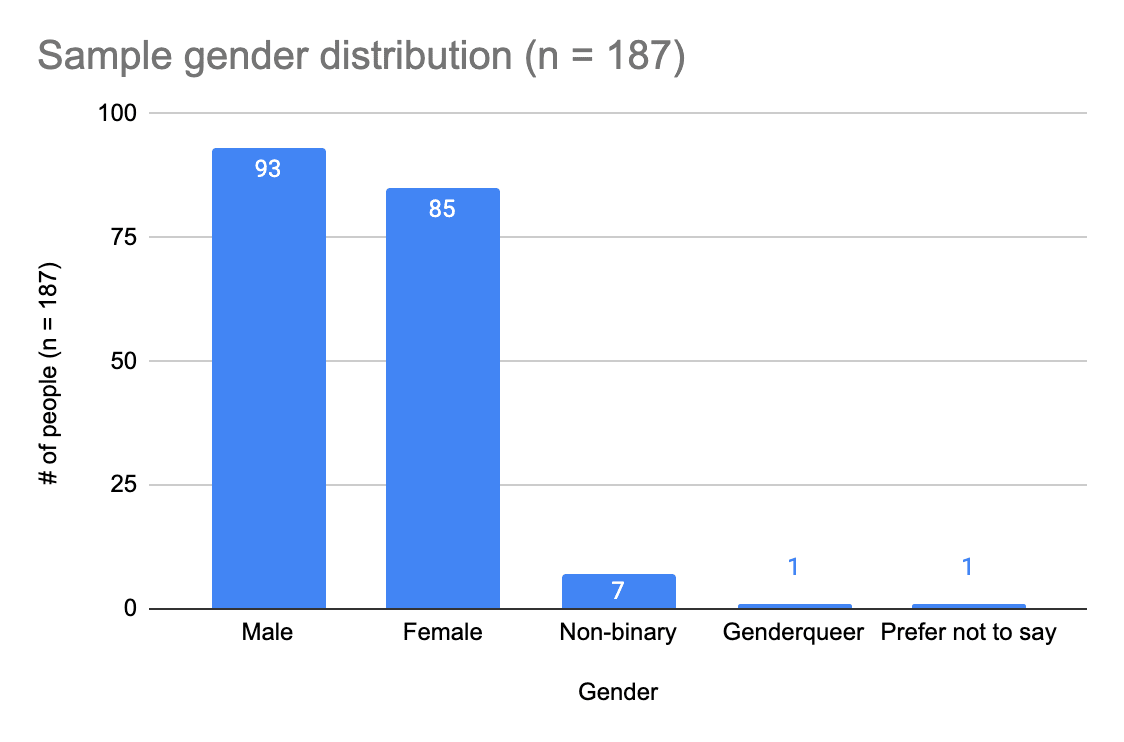
(2) Gender
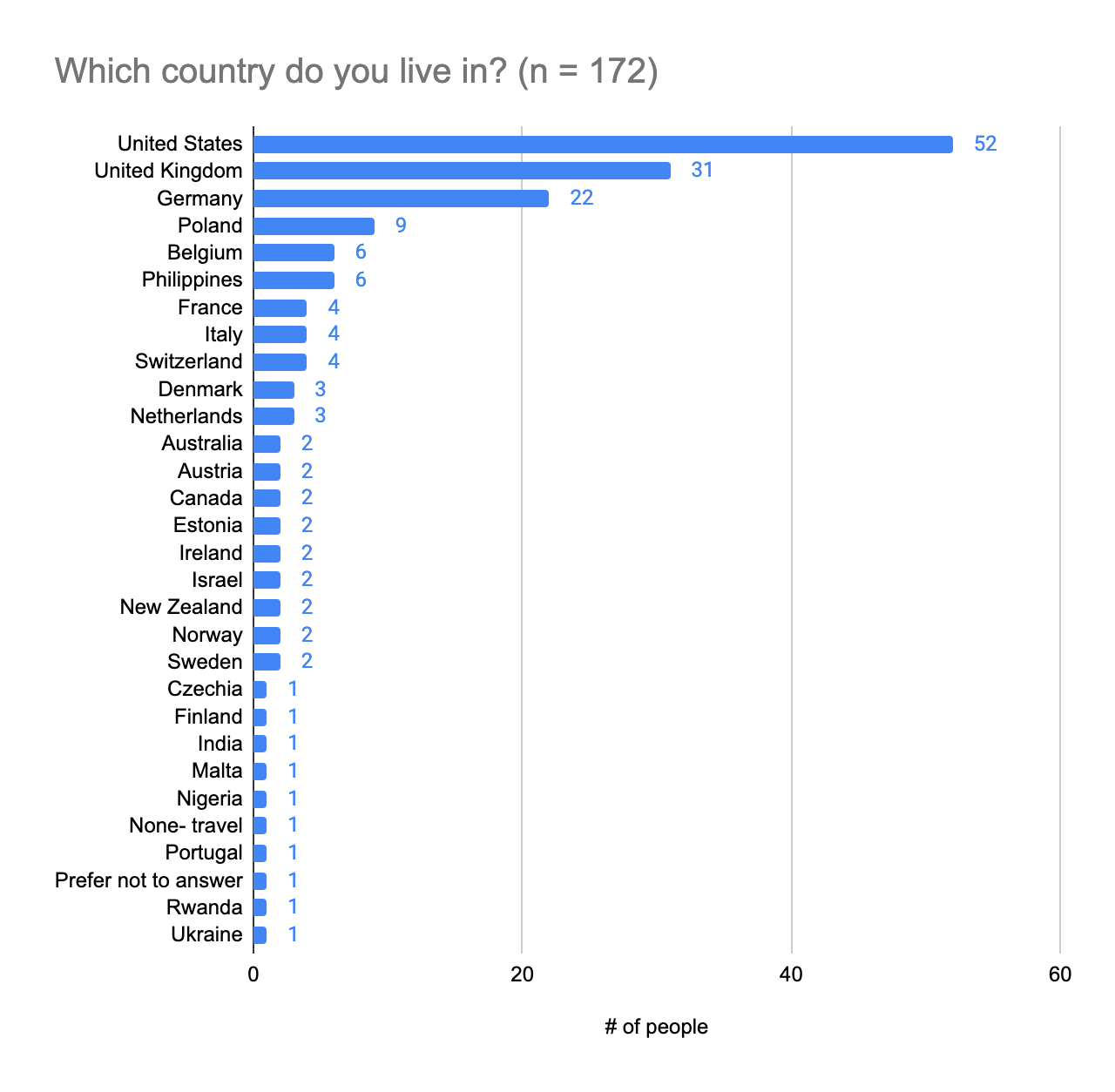
(3) Country of residence
The majority of survey participants are based in the United States and United Kingdom.
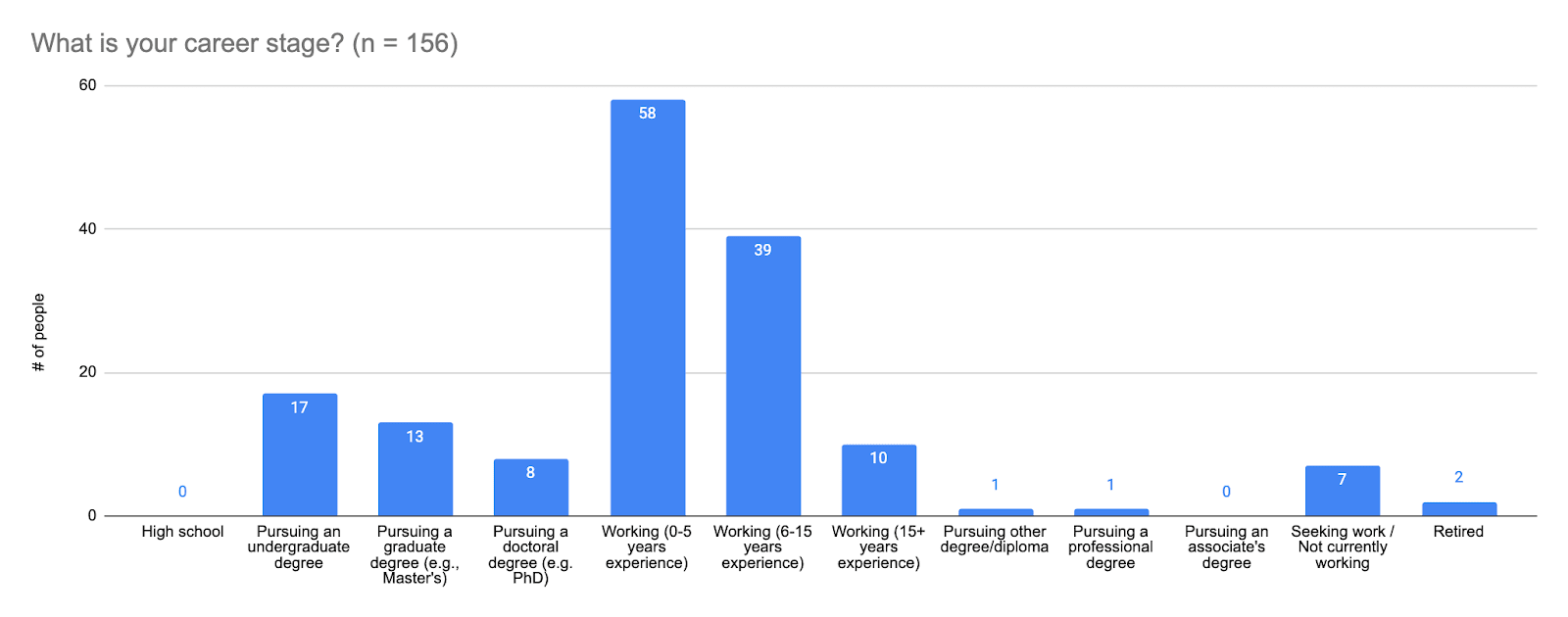
(4) Career stage
Answer choices from left to right are:
- High school
- Pursuing an undergraduate degree
- Pursuing a graduate degree (e.g., Master's)
- Pursuing a doctoral degree (e.g., PhD)
- Working (0-5 years experience)
- Working (6-15 years experience)
- Working (15+ years experience)
- Pursuing other degree / diploma
- Pursuing a professional degree
- Pursuing an associate's degree
- Seeking work / Not currently working
- Retired
Most survey participants are working and have 0-15 years' work experience.
(5) Engagement with Effective Altruism
Answer choices were defined as follows:
- No engagement: I’ve heard of Effective Altruism, but do not engage with Effective Altruism content or ideas at all
- Mild: I’ve engaged with a few articles, videos, podcasts, discussions, events on effective altruism (e.g. reading Doing Good Better or spending ~5 hours on the website of 80,000 Hours)
- Moderate: I’ve engaged with multiple articles, videos, podcasts, discussions, or events on Effective Altruism (e.g. subscribing to the 80,000 Hours podcast or attending regular events at a local group). I sometimes consider the principles of effective altruism when I make decisions about my career or charitable donations.
- Considerable: I’ve engaged extensively with Effective Altruism content (e.g. attending an EA Global conference, applying for career coaching, or organizing an EA meetup). I often consider the principles of Effective Altruism when I make decisions about my career or charitable donations.
- High: I am heavily involved in the Effective Altruism community, perhaps helping to lead an EA group or working at an EA-aligned organization. I make heavy use of the principles of Effective Altruism when I make decisions about my career or charitable donations.
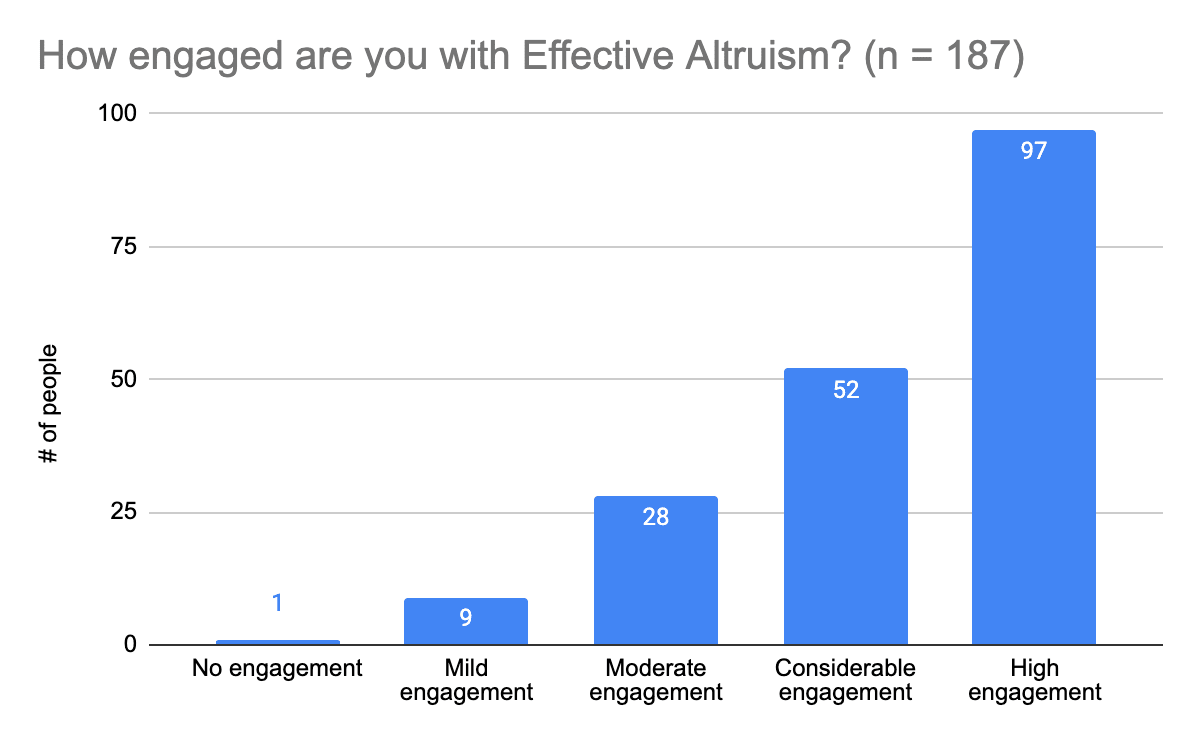
Most survey participants are fairly engaged with Effective Altruism (considerable to high engagement).
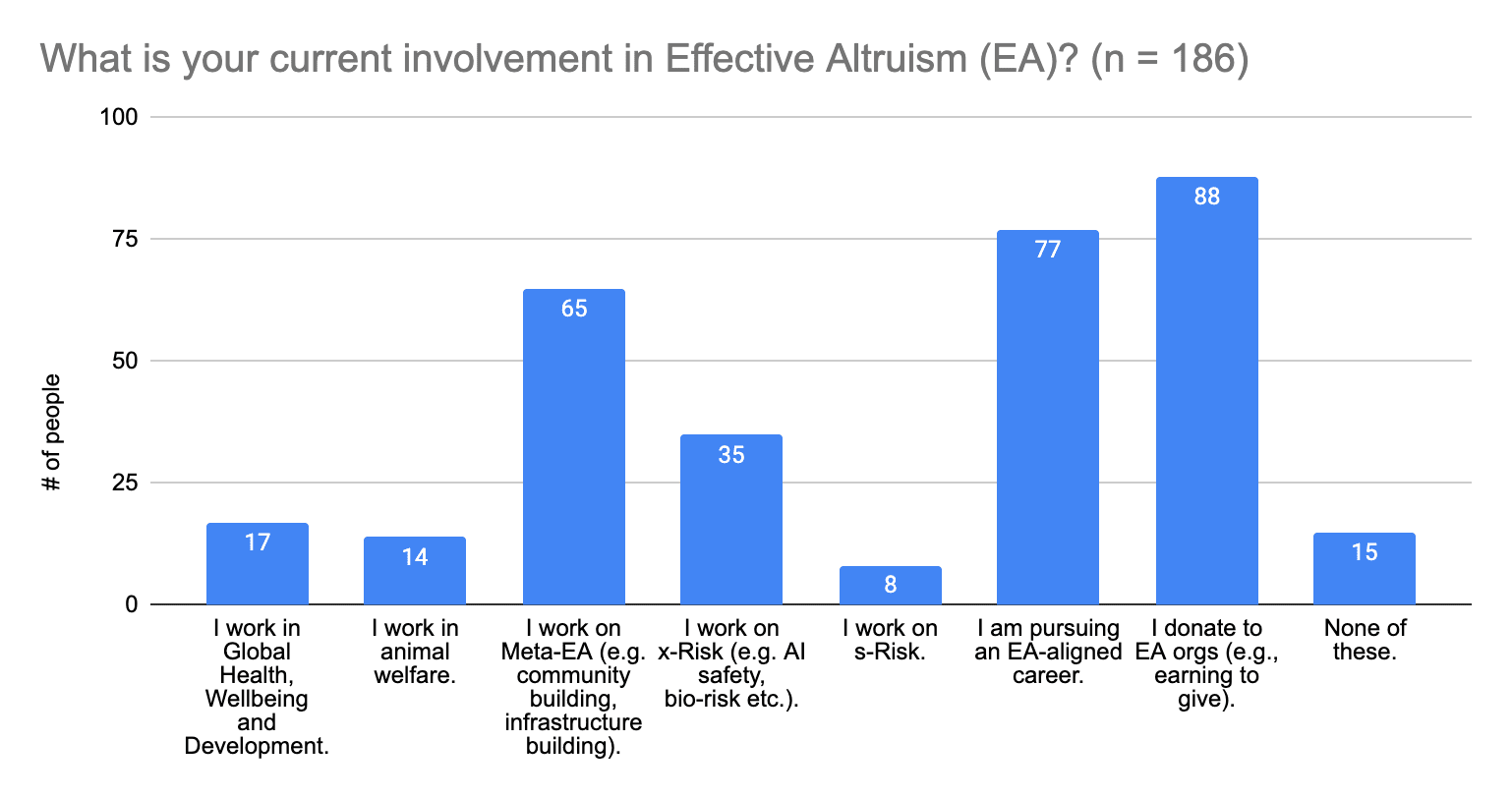
(6) Current involvement in Effective Altruism
People who answered this question could provide multiple answers, so survey participants who are involved in multiple sectors provided multiple answers.
Mental Health Topics and DisordersMental Health Topics and Disorders
This section was geared toward getting a more granular view of what community members struggle with in terms of their mental health. Building off of lessons learned from the 2021 EA Mental Health Survey, the questions are structured to provide more extensive lists of options for people to choose from, and to make the distinction between mental health disorders and mental health topics (which can include symptoms of disorders).
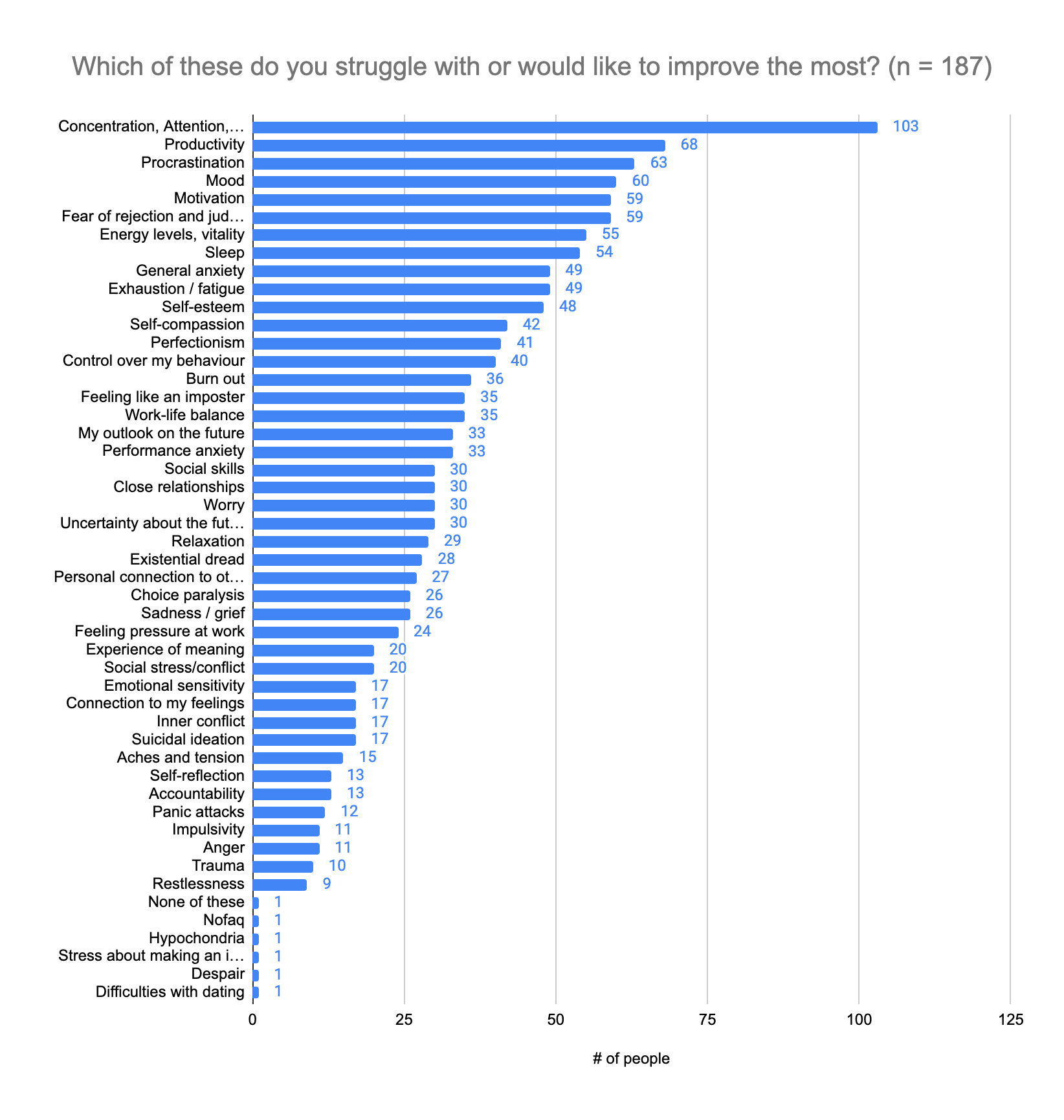
(1) Topics people struggle with or would like to improve the most
People struggle the most with concentration, attention, and focus (n =103; 55%), followed by productivity (n = 68; 36%) and procrastination (n = 63; 34%). The topics with ellipses are:
- Concentration, Attention, Focus
- Fear of rejection and judgment by others
- Uncertainty about the future
- Personal connection to other members of the community
- Stress about making an impact with my career
Please note: People who answered this question could provide multiple answers.
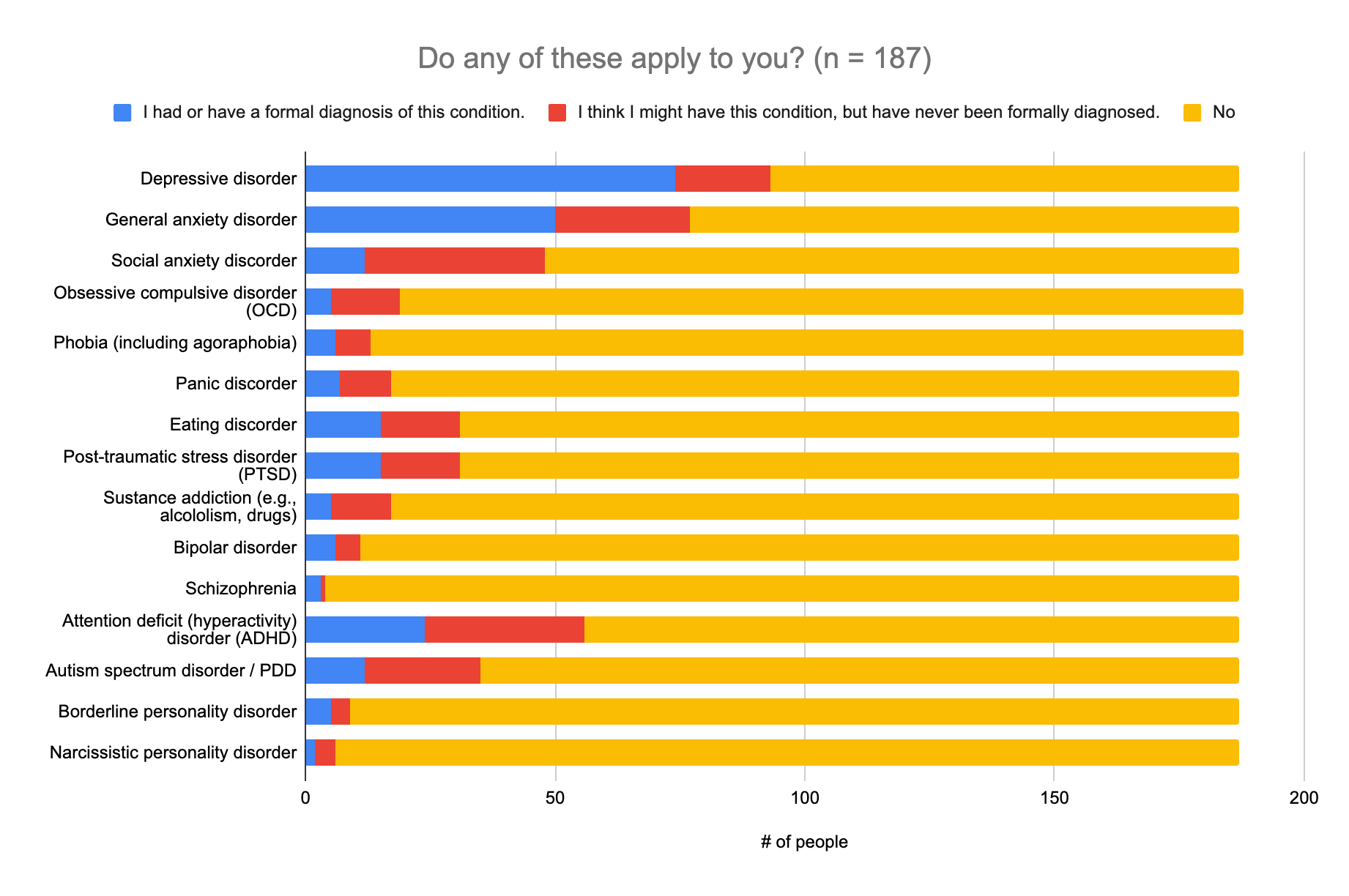
 (2) Applicable categories of disorders
(2) Applicable categories of disorders
This question was meant to get a better idea of the prevalence of diagnosed and suspected mental health struggles in the community, and listed out categories of disorders as defined in the DSM-V. The distinction in this question is important for determining what kind of help people will be able to access (which can depend on having a diagnosis), and therefore determining how to prioritize what information is needed.
 (3) Other disorders and conditions
(3) Other disorders and conditions
Other disorders (or suspected disorders) and conditions provided were:
- Seasonal affective disorder
- Sleep disorder
- Migraines
- Obsessive Compulsive Personality Disorder (this is not the same as OCD)
- Chronic Fatigue Syndrome
- Irritable Bowel Syndrome (stress induced)
- Nonverbal Learning Disorder
Answers that were reclassified and added to Question 2, based on the DSM-V were:
- Body-focused repetitive behaviors (BFRB), which is classed as an Obsessive Compulsive Disorder
- Vehophobia, which is a phobia
Summary of Results
The top three symptoms or topics people struggle the most with are concentration, attention, and focus (n =103; 55%), followed by productivity (n = 68; 36%) and procrastination (n = 63; 34%). Over a quarter of those surveyed (n = 50+; 27%) have been diagnosed with a depressive disorder, an anxiety disorder, or ADHD, or feel that they have a disorder that falls into one of these categories, but have not been diagnosed. It would therefore probably be helpful to focus on providing more information on dealing with or finding support for anxiety, depression, and ADHD, and improving one’s concentration, attention, focus, and productivity, as well overcoming procrastination.
State of Your Mental Well-Being
This section was designed to gauge the state of mental well-being across the wider community, and satisfaction with one's life, relationships, community, and productivity.
(1) Life satisfaction (x̄=6.6, SD=2.0)
Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”.
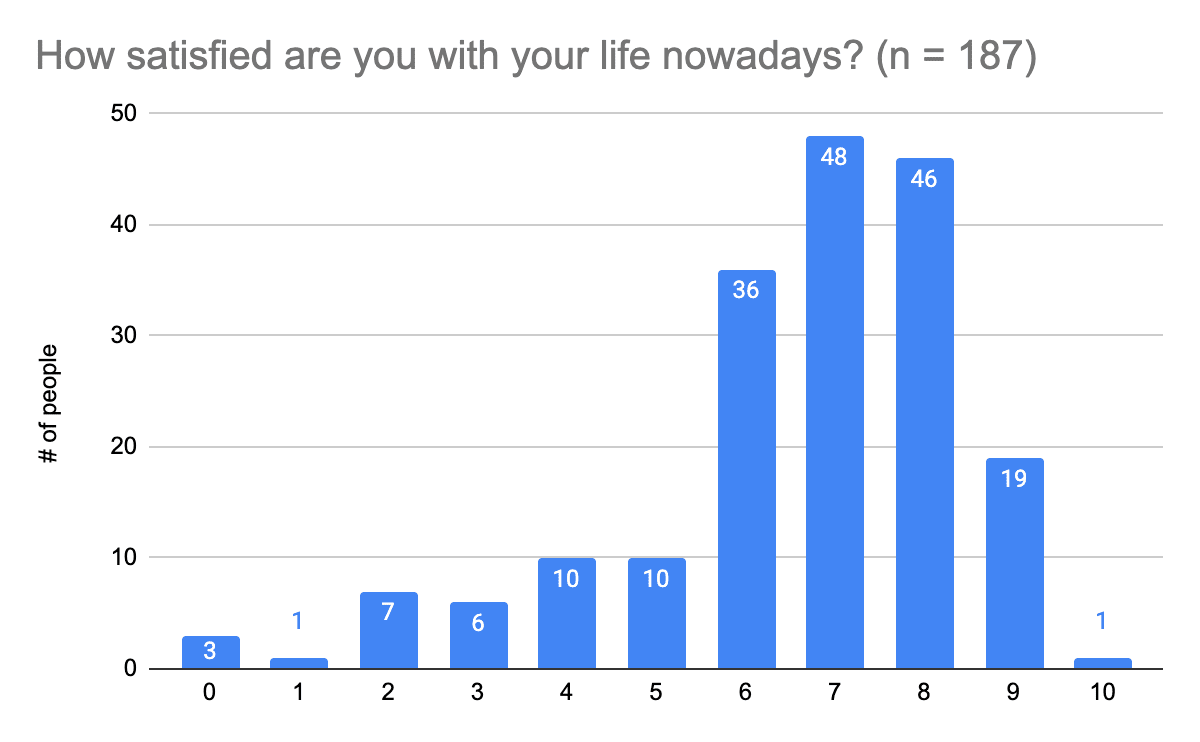
We used the same question that was asked in the report ‘Personal and economic wellbeing' by the Office of National Statistics, and in 2018 the average overall life satisfaction in the EU was 7.3, while in our survey it was 6.6. The life satisfaction of people in the EA community who filled out this survey in 2023 seems to be lower than the one of the typical EU member in 2018, and is similar to the one of people in Greece or Hungary (see Figure 1).
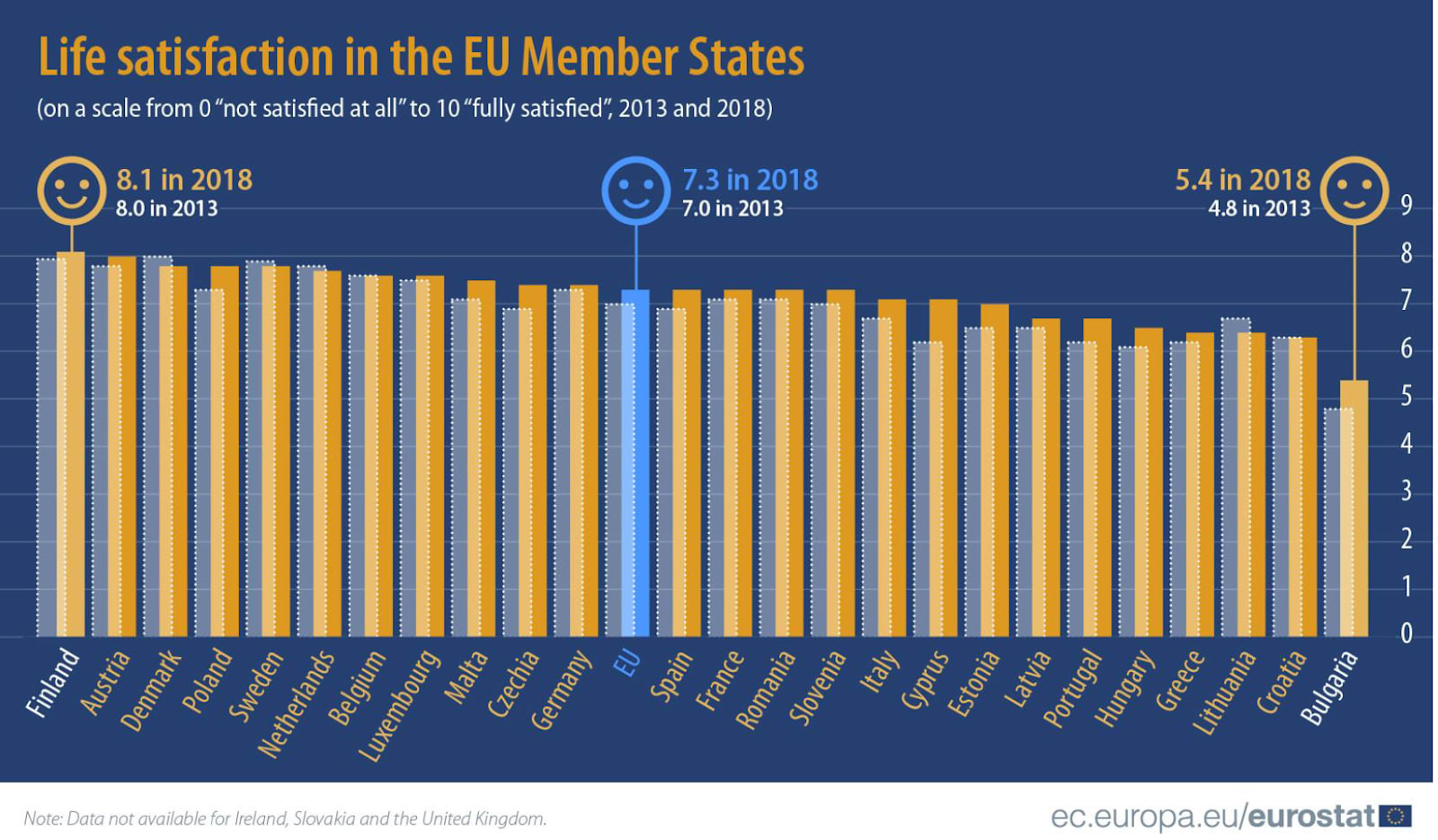
Figure 1. Results of the report Personal and economic wellbeing
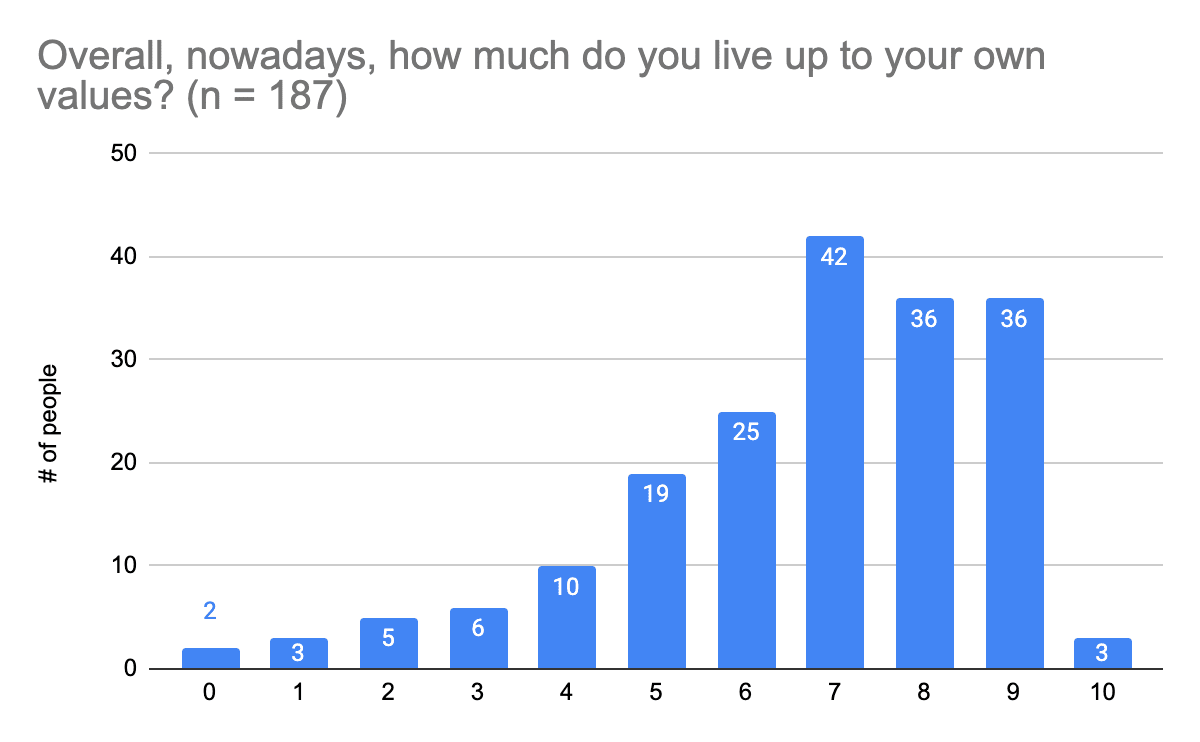
(2) Living up to one's values (x̄=6.7, Mdn.=7.0 SD=2.1)
Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”.
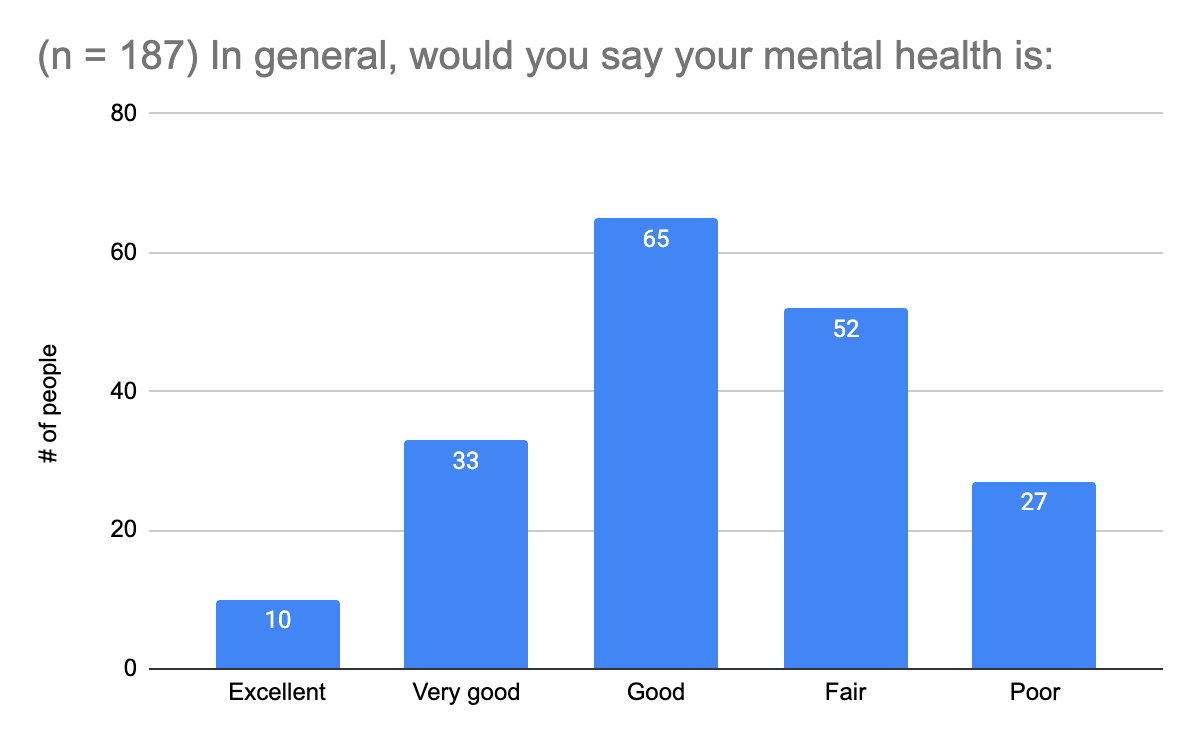
 (3) Mental health status
(3) Mental health status
We asked a single standardized item question to self-rate mental health (the SRMH). In this scoping review (2014), you can find out more about the item, correlates, and applications.
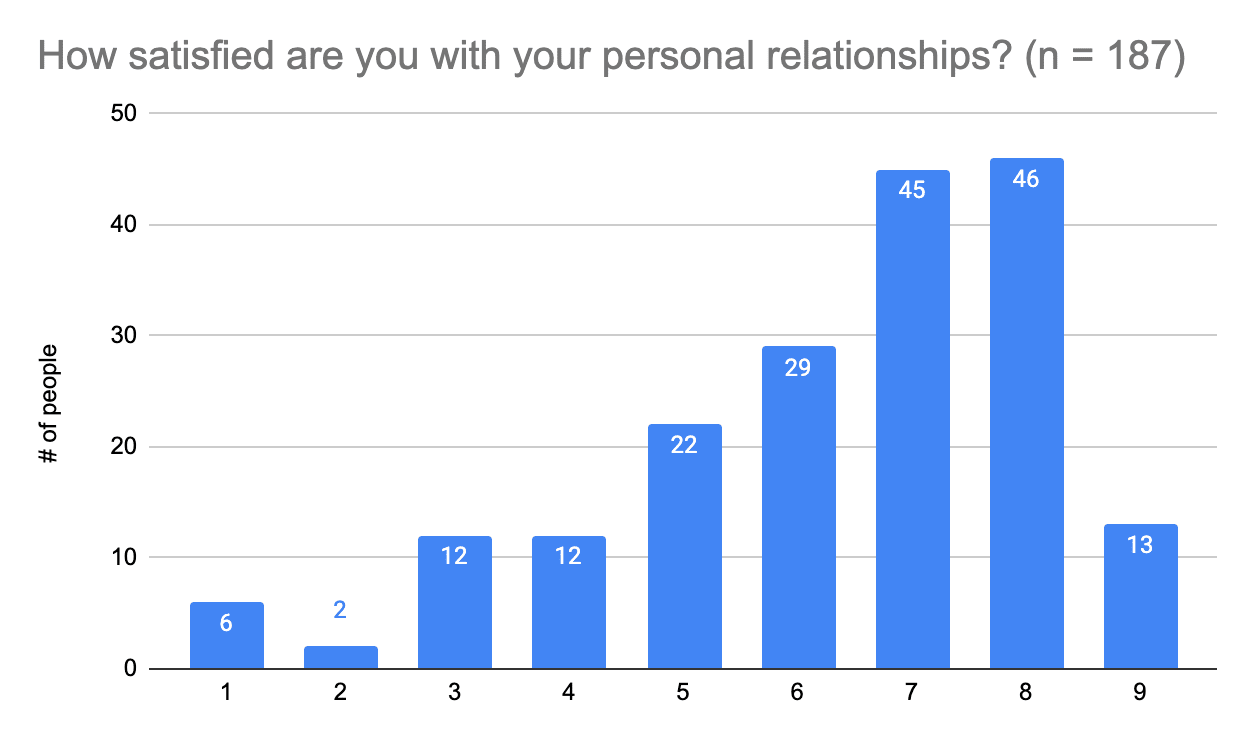
(4) Satisfaction with personal relationships (x̄ =6.3, SD=1.9)
Answers to this question were on a scale of 1 to 9, where 1 was “Very dissatisfied” and 9 was “Very satisfied”.
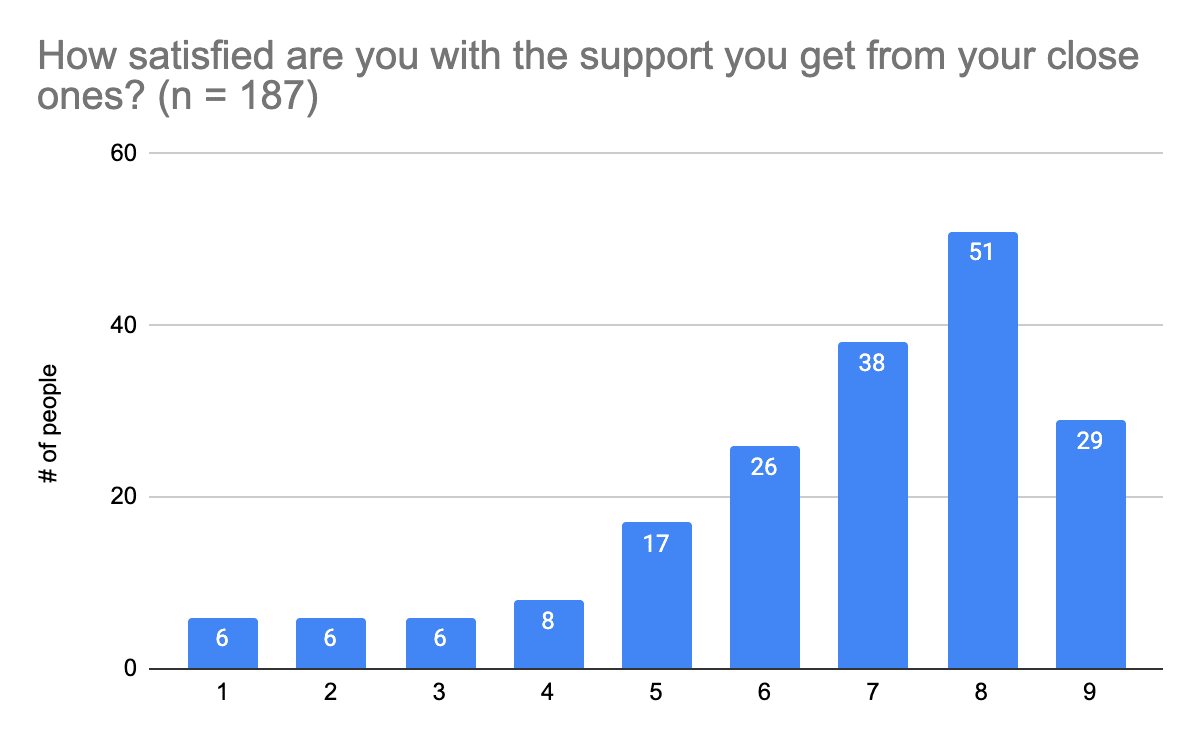
 (5) Satisfaction with support in close personal relationships (x̄=6.7, Mdn.=7.0 SD=2)
(5) Satisfaction with support in close personal relationships (x̄=6.7, Mdn.=7.0 SD=2)
Answers to this question were on a scale of 1 to 9, where 1 was “Very dissatisfied” and 10 was “Very satisfied”.
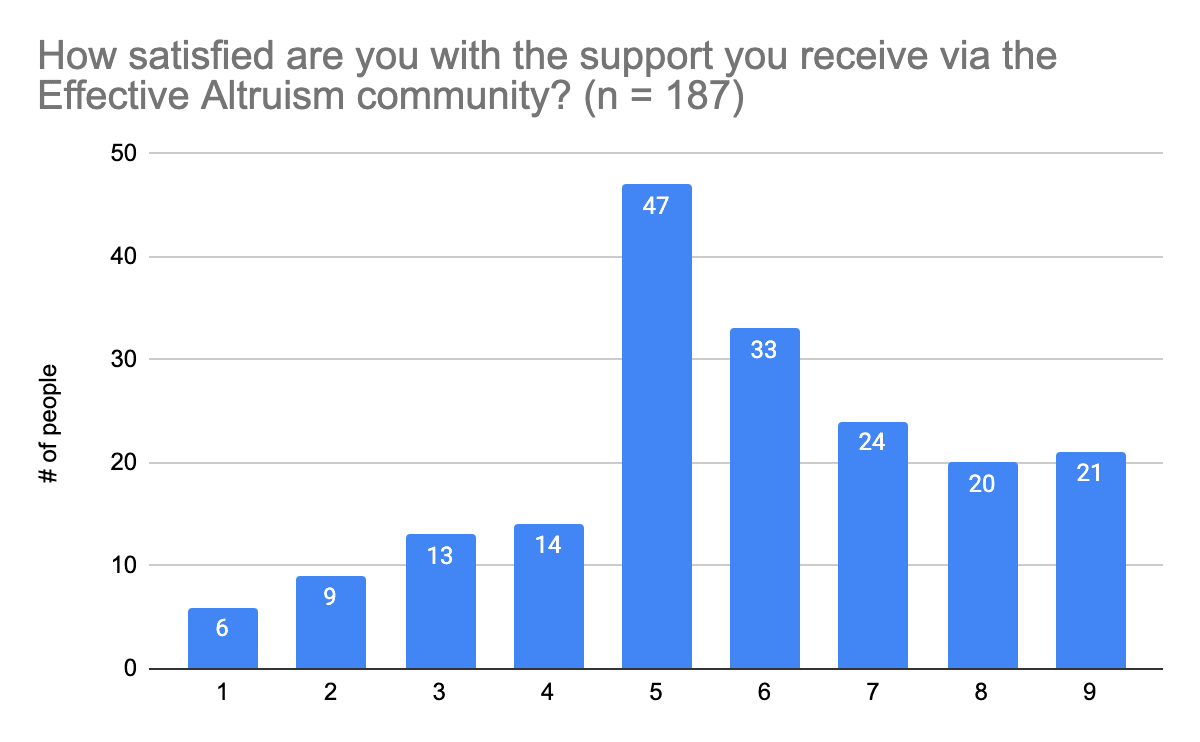
 (6) Satisfaction with support from the Effective Altruism community (x̄=5.7, SD=2.1)
(6) Satisfaction with support from the Effective Altruism community (x̄=5.7, SD=2.1)
Answers to this question were on a scale of 1 to 9, where 1 was “Strongly disagree” and 9 was “Strongly agree”.
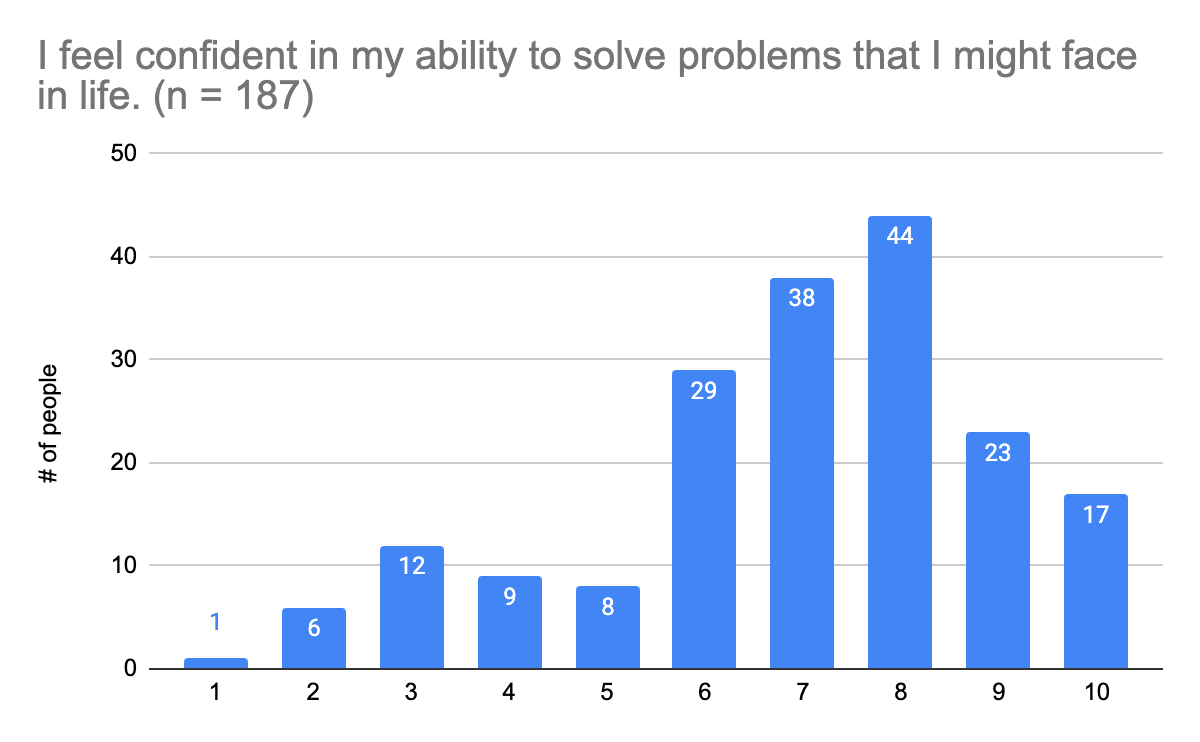
(7) Confidence ability to solve life problems (x̄=6.9, SD=2.1)
Answers to this question were on a scale of 1 to 10, where 1 was “Very dissatisfied” and 10 was “Very satisfied”. We used this standardized single item to measure self-efficacy. Find out more about the item in the corresponding paper (2016) here.
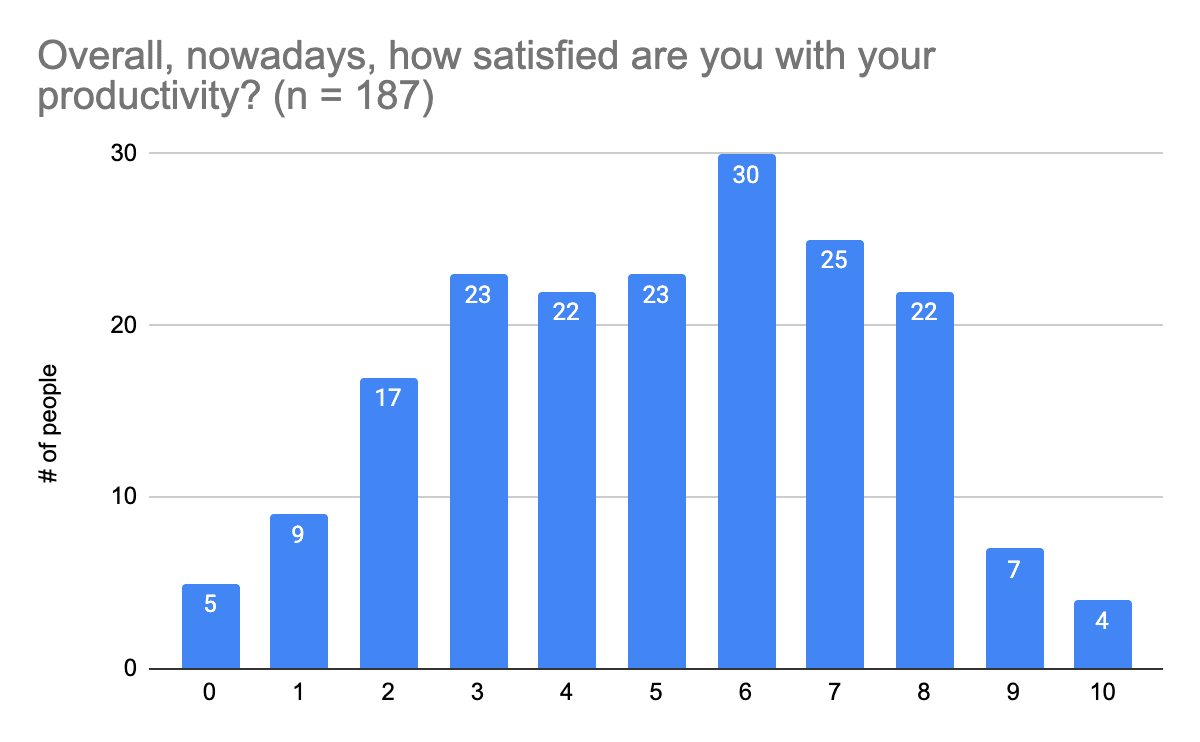
 (8) Satisfaction with productivity (x̄=5.1, SD=2.4)
(8) Satisfaction with productivity (x̄=5.1, SD=2.4)
Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”. Satisfaction with productivity seems to be much lower than satisfaction with relationships and general life in the EA community members who took part in this survey.
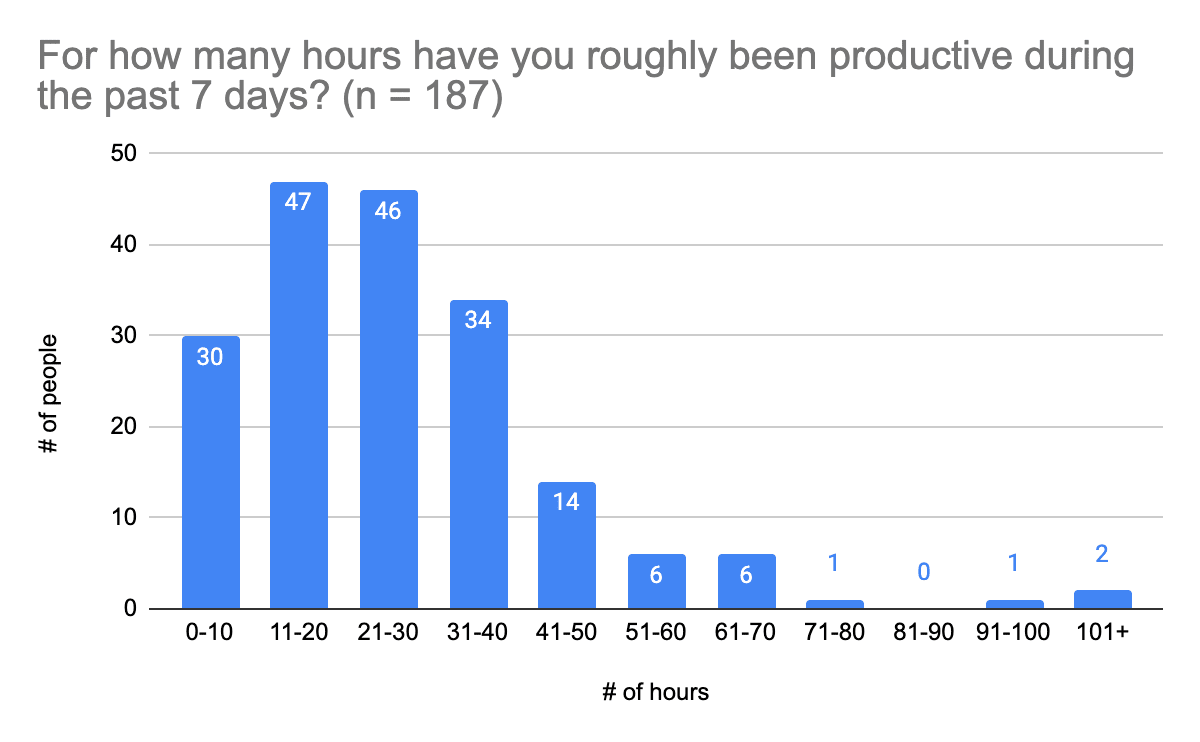
(9) Estimate of actual productivity (x̄=29.4, SD=25.5)
This was a free-form response, so answers have been grouped into units of 10.
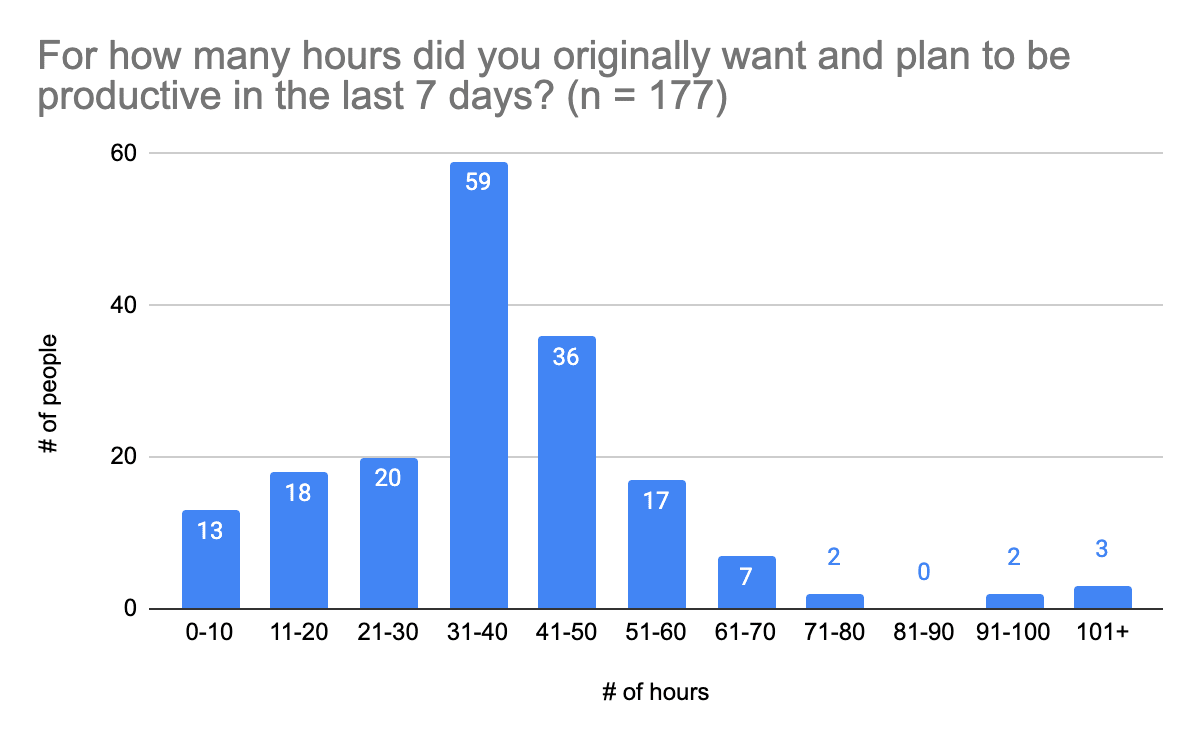
(10) Estimate of planned productivity (x̄=41.1, SD=26.2)
This was a free-form response, so answers have been grouped into units of 10.
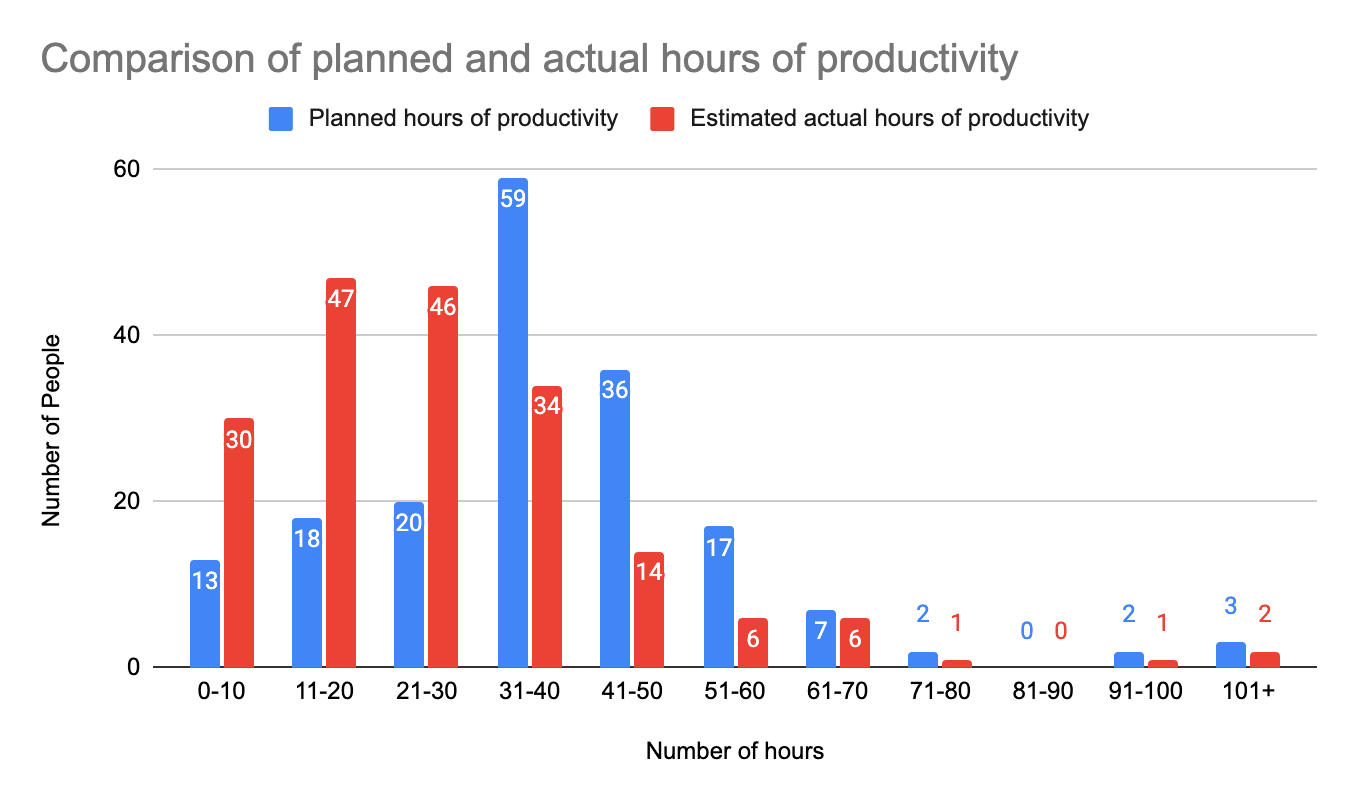
Visual comparison of planned versus actual hours of productivity:
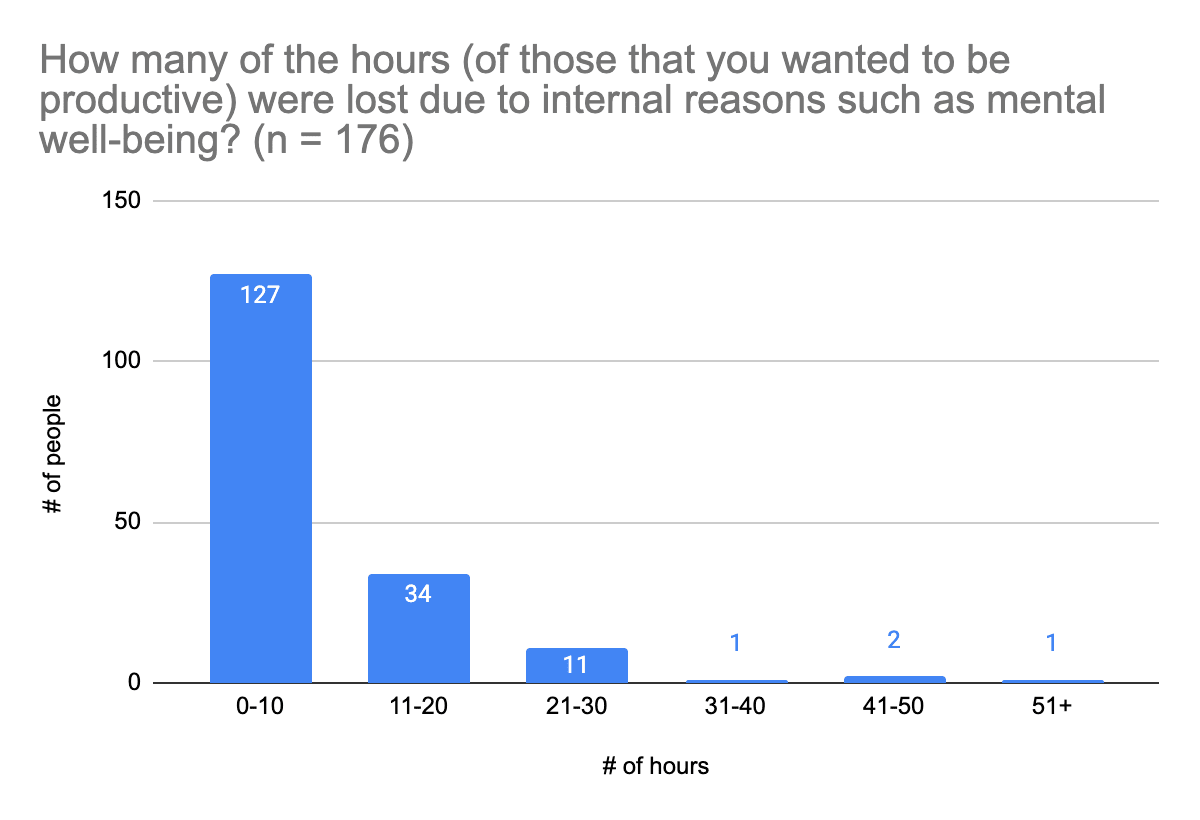
(11) Hours lost due to internal reasons, such as mental well-being (x̄=10.5, SD=22.2)
The results mean that people who filled out the survey estimated that they worked nearly 15 hours less than they had planned (x̄=14.9), and for roughly ⅔ of survey participants, two out of 3 hours were lost due to mental wellbeing or other internal reasons.
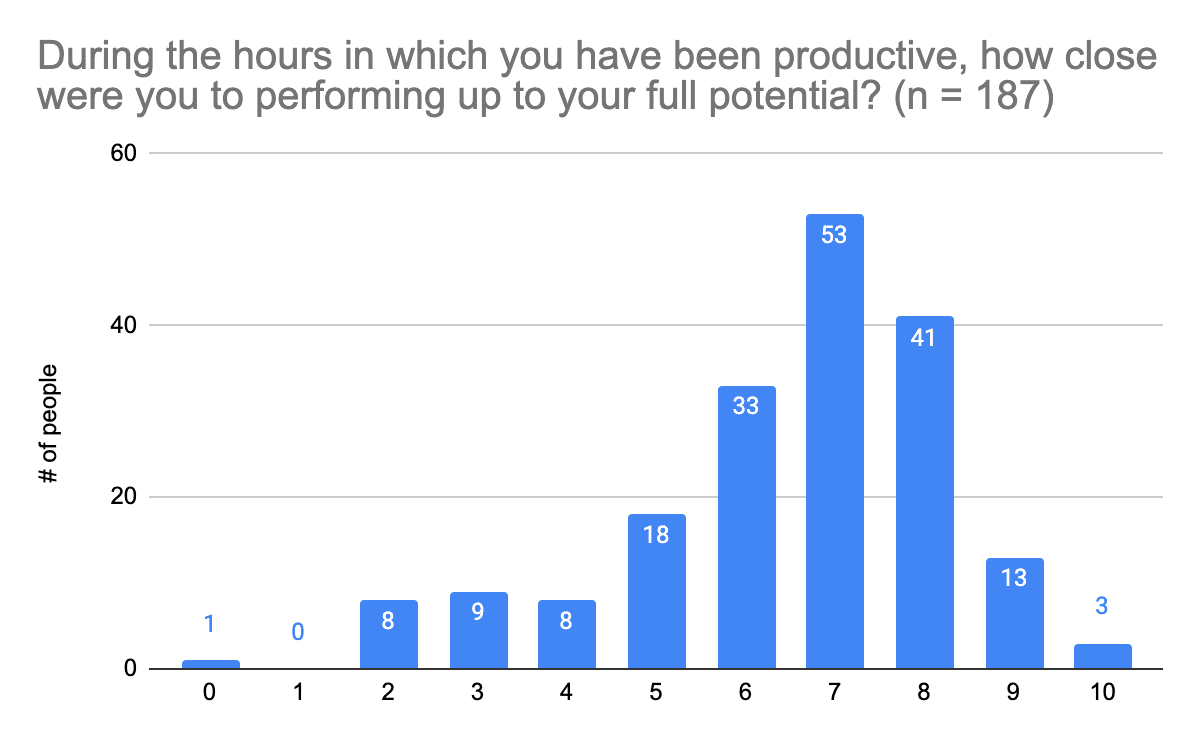
(12) Estimate of productive hours that were close to performing up to one's full potential (x̄=65%, SD=19%)
Answers to this question were on a scale of 0 to 10, where 0 was 0% and 10 was 100%.
Summary of Results
Most people who completed this survey (n = 130; 70%) are generally satisfied with their lives nowadays (scores of 6-8 out of 10), but a few people (n = 20; 11%) are very satisfied (scores of 9 or 10). Similarly, most survey participants generally feel that they live up to their values (scores of 7-9 out of 10, n = 114; 61%), and would say their mental health is “good” or better (n = 108; 58%). Those who completed this survey are generally satisfied in their relationships (score 7+ out of 9, n = 104; 56%) and the support they get from their loved ones (score 7+ out of 9, n = 118; 63%). Most survey participants are generally somewhat satisfied with the support they get from the Effective Altruism community (score of 5-7 on 9-point scale, n = 104; 56%). So people generally experience good mental health and feel supported, but that doesn’t mean there isn’t room to improve life satisfaction and well-being, and increase feelings of support (especially given the information provided in the Demand for Interventions section of this post).
People appear to mostly be somewhat confident in their abilities to solve problems they face in life (score of 6 to 9 on 10-point scale, n = 134; 72%), and somewhat satisfied with their overall levels of productivity (score of 5 or above on 10-point scale, n = 111; 59%). Most survey participants were productive for up to 40 hours in a week (n = 157; 84%), though a lot of people were not as productive as they would have liked. A majority of participants (n = 112; 63%) aimed to be productive for 31-60 hours in a week; 54 people (31%) achieved this. Most survey participants lost up to 10 hours of productivity due to reasons related to mental well-being (n = 127; 72%). Most participants (though not all) also felt they were somewhat close to reaching their full potential during the hours in which they were productive (score of 6 or above on 10-point scale, n = 143; 76%); few felt they reached their full potential (score of 9+, n = 16; 9%). So it could be beneficial to provide people with information on improving their productivity, especially since this is a topic a lot of people (n = 68; 36%) said they struggle with.
Experience with Interventions
This section was included to get a better idea of the types of mental health interventions community members have tried, including various types of behavioral interventions, therapeutic methods, and substances.
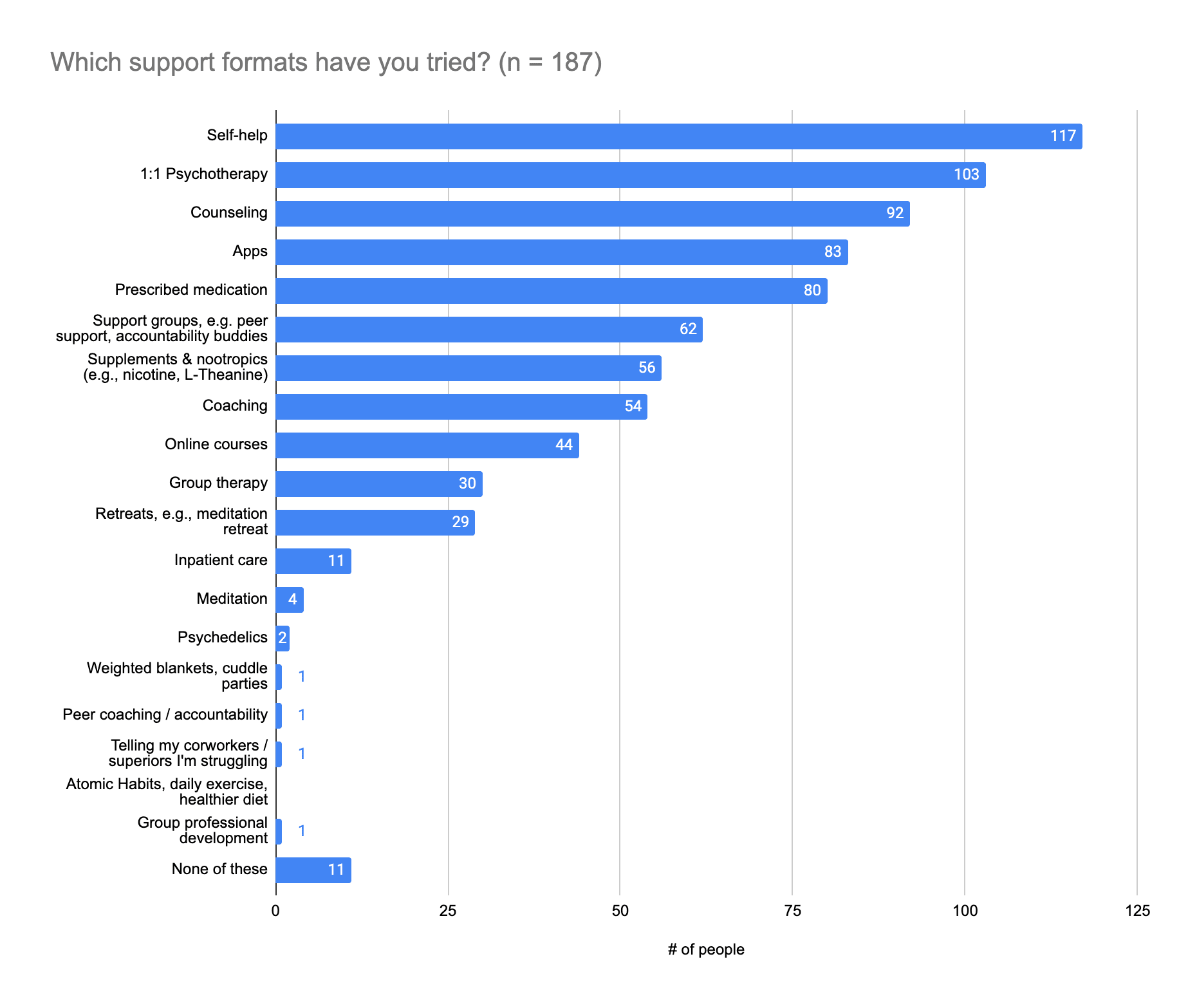
(1) Support formats tried
Please note: People who answered this question could provide multiple answers.
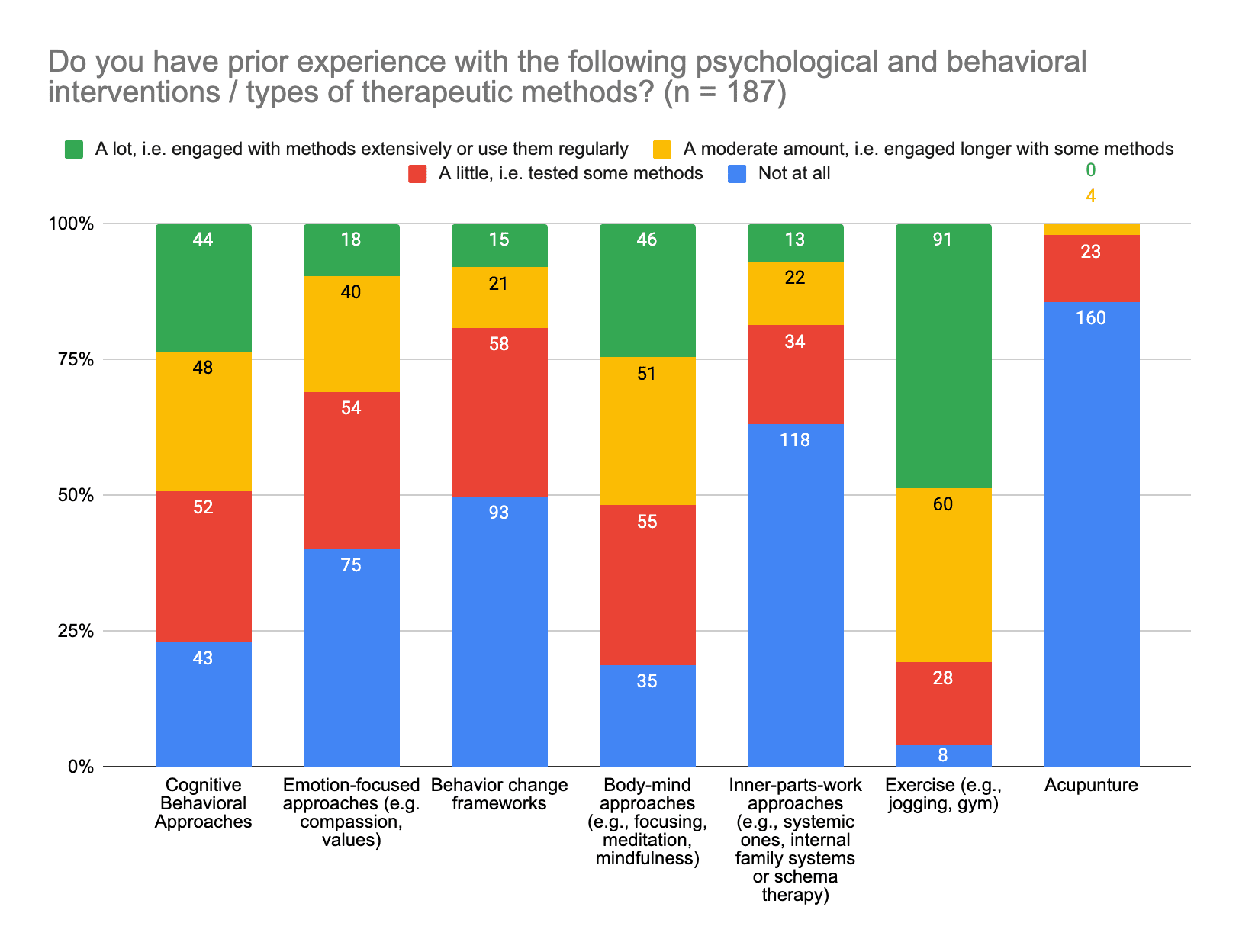
(2) Experience with psychological and behavioral interventions / types of therapeutic methods
Please note: Numbers above the chart are associated with the color groups in the respective columns. Also, people who answered this question could provide multiple answers.
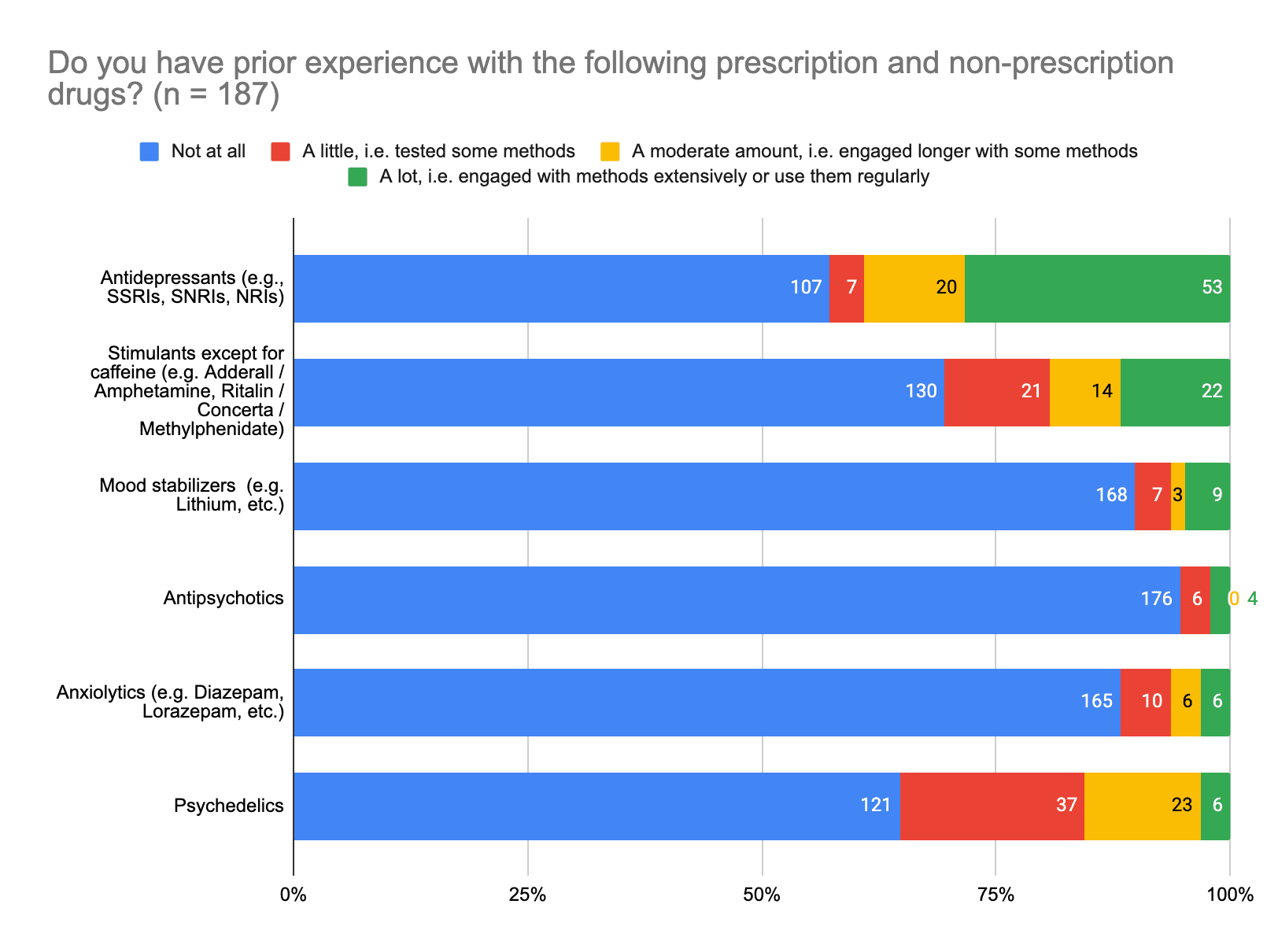
(3) Experience with various prescription and non-prescription drugs
Categories were (top to bottom of chart):
- Antidepressants (e.g., SSRIs, SNRIs, NRIs)
- Stimulants except for caffeine (e.g. Adderall / Amphetamine, Ritalin / Concerta / Methylphenidate)
- Mood stabilizers (e.g. Lithium, etc.)
- Antipsychotics
- Anxiolytics (e.g. Diazepam, Lorazepam, etc.)
- Psychedelics
Please note: Numbers to the right margin of the chart are associated with the color groups in the respective rows. Also, people who answered this question could provide multiple answers.
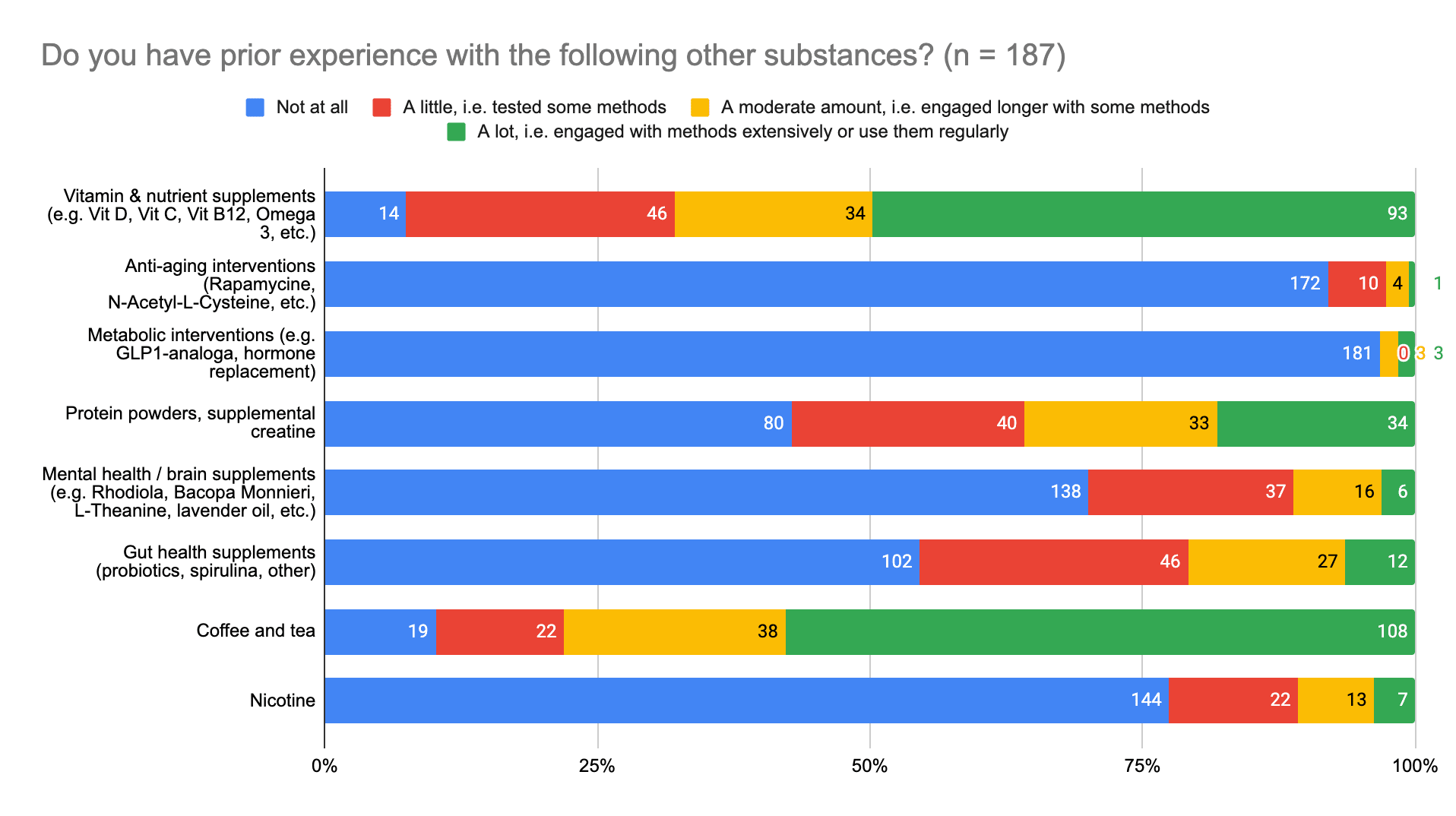
(4) Experience with various other substances
Please note: Numbers to the right margin of the chart are associated with the color groups in the respective rows. Also, people who answered this question could provide multiple answers.
Categories were (top to bottom of chart):
- Vitamin & nutrient supplements (e.g. Vit D, Vit C, Vit B12, Omega 3, etc.)
- Anti-aging interventions (Rapamycine, N-Acetyl-L-Cysteine, etc.)
- Metabolic interventions (e.g. GLP1-analoga, hormone replacement)
- Protein powders, supplemental creatine
- Mental health / brain supplements (e.g. Rhodiola, Bacopa Monnieri, L-Theanine, lavender oil, etc.)
- Gut health supplements (probiotics, spirulina, other)
- Coffee and tea
- Nicotine
(5) Experience with other forms of interventions
There was at least one response for each of the following:
- Daily use of productivity apps (FocusMate, BeeMinder, Google Calendar)
- Habit-tracking
- Journaling, checking-in with oneself, gratitude & compassion exercises, etc.
- Social events (being taken by friends or attending on one's own)
- Venting to friends, peers, or counselors
- Pets
- Dawn simulator, light exposure in the mornings
- Melatonin
- Consistently doing things to improve sleep (e.g., keeping room cool and dark, earplugs, sleeping mask, avoid/dim light in the evening, antihistamines)
- Ioniser
- Sound therapy
- Music
- Art
- Going for regular walks
- Yoga
- Meditation
- Monastic life
- Cold showers
- Massage
- Working part-time
- Pushing through and getting things done
- Dialectical Behavior Therapy (DBT)
- Meta-cognitive therapy
- Authentic Relating practices
- Occupational therapy
- Acceptance and Commitment Yherapy
- Hypnotherapy
- Electro-convulsive therapy
- Long-term psychodynamic psychotherapy
- Gestalt therapy
- Anticonvulsants as adjunctive pharmacotherapy (lamotrigine, pregabalin)
- Modafinil
- Ketamine (IV)
- NVC, high dose EPA without DHA
- Ashwagandha
- Kratom
- CBD oils
- Cannabis
- Photobiomodulation
Summary of Results
The support formats most survey participants have tried are self-help (n = 117; 63%), 1:1 psychotherapy (n = 103; 55%), and counseling (n = 92; 49%). The next most popular were apps (n = 83; 44%) and prescribed medication (n = 80; 43%). It could therefore be helpful to provide people with information on support formats with which they are less familiar, such as support groups (n = 62; 33%), supplements and nootropics (n = 56; 30%), coaching (n = 54; 29%), online courses (n = 44; 24%), and atomic habits and other lifestyle changes, such a healthy diet and use of weighted blankets.
In terms of behavioral and psychological interventions, survey participants have engaged at least a little with exercise (n = 179; 96%), body-mind approaches (e.g., focusing, meditation, mindfulness) (n = 152; 81%), and cognitive behavioral approaches (n = 144; 77%), but not much with acupuncture and inner-parts-work (e.g., systemic methods, internal family systems or schema therapy). It might be a good idea then to provide information about these less popular approaches, as well as emotion focused approaches and behavior change frameworks, both of which some people have tested (n = 54 (29%) and 58 (31%), respectively), but fewer people have used (n = 58 (31%) and 36 (19%) respectively).
Most survey participants have had at least a little experience with antidepressants (n = 80; 43%) and stimulants (n = 57; 30%), and no experience with antipsychotics (n = 176; 94%), mood stabilizers (n = 168; 89%), and anxiolytics (n = 165; 88%). It might therefore be useful to point people to resources where they can access medical literature and medical support on these topics, should they wish to know more.
Most people have at least a little experience with vitamins and nutrient supplements (n = 173; 93%) and coffee and tea (n = 168; 90%), but not any with anti-aging interventions (n = 172; 92%) and metabolic interventions (n = 181; 97%). It might be helpful to provide information on substances people have no experience with, or have tested or used a moderately, though not extensively, such as protein powders and supplemental creatine (n = 73; 39%), mental health / brain supplements (e.g., Rhodiola, Bacopa Monnieri, L-Theanine, lavender oil) (n = 53; 28%), and gut health supplements (e.g., probiotics, spirulina) (n = 73; 39%), so that people can make more informed decisions about these substances, and whether or not they’d be helpful to them.
Demand for Interventions
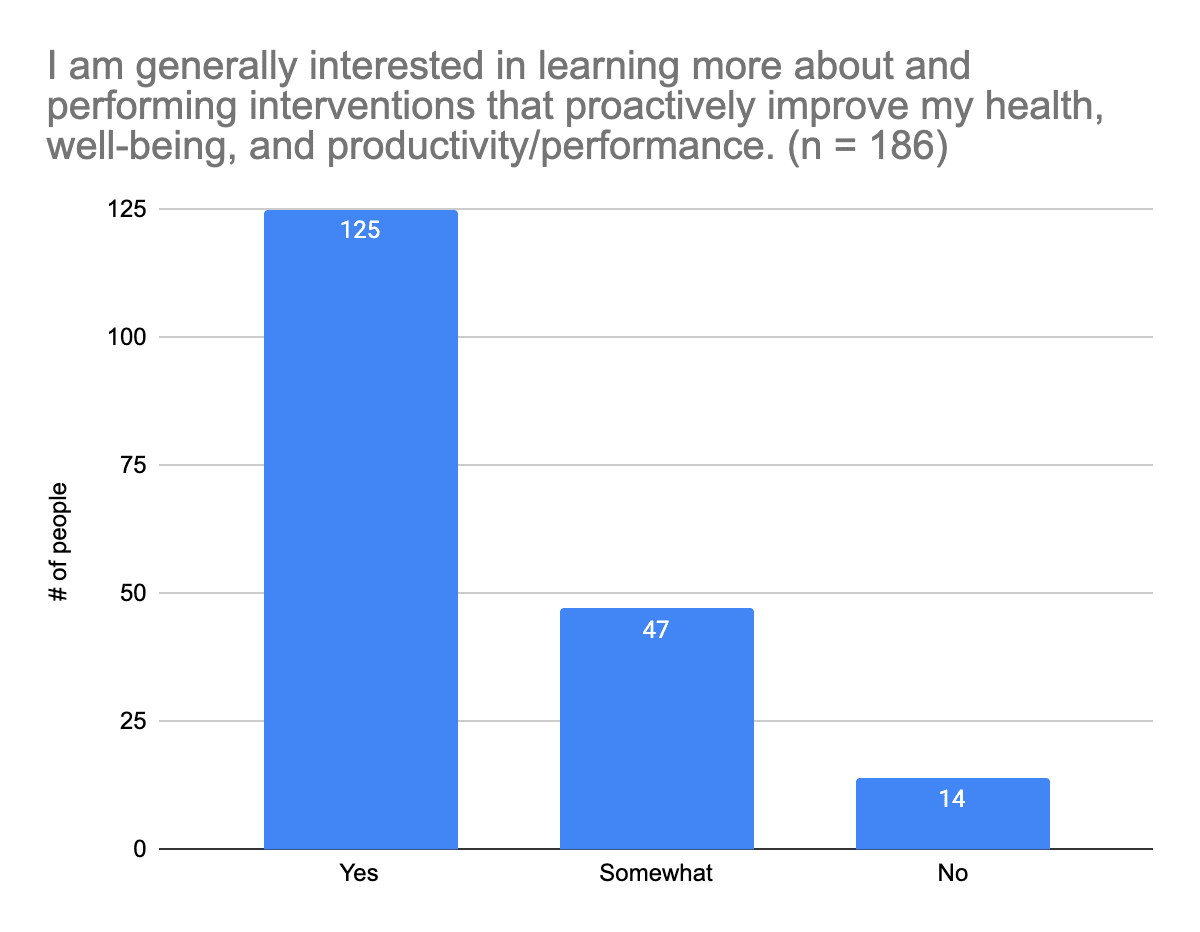
(1) Interest in learning more about and using various health, well-being, and productivity interventions
This included everything from lifestyle changes (e.g. better sleep), behavioral techniques (e.g. meditation), supplements (e.g. Omega 3, vitamins), nootropics (e.g. L-Theanine, Bacopa Monnieri), drugs (e.g. Ritalin / Concerta), to biohacking (e.g. hormone replacement).
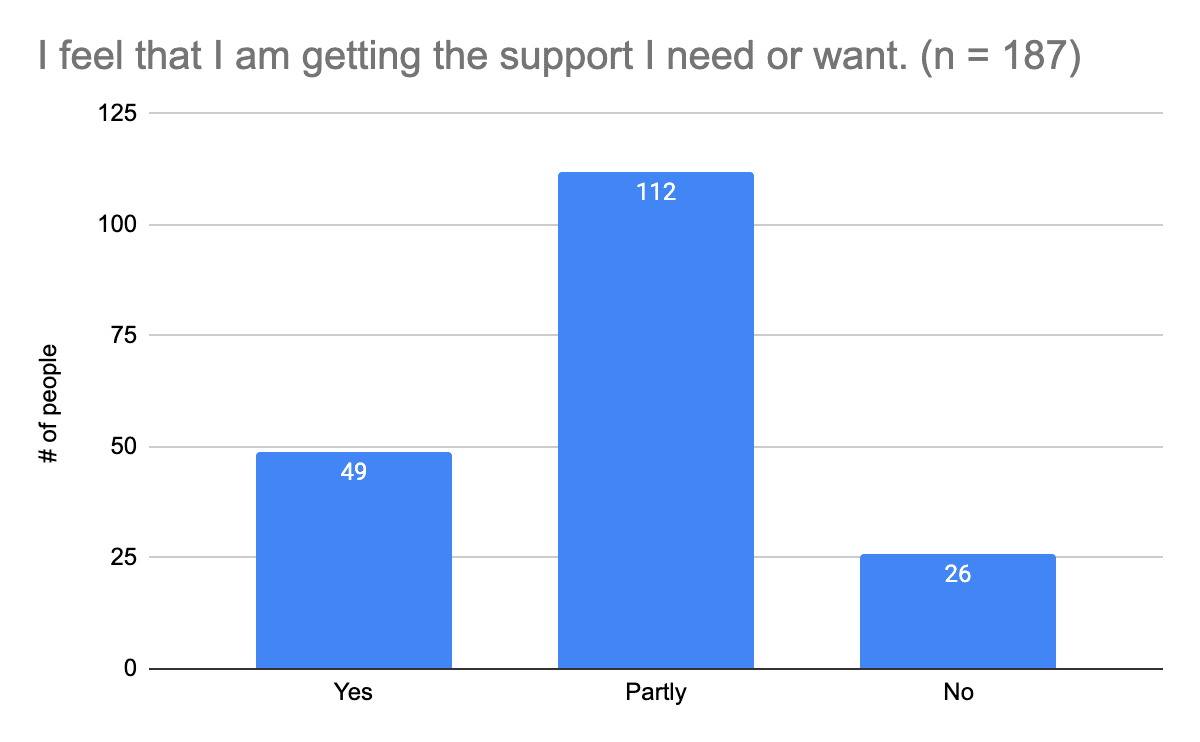
(2) Whether people feel they receive their desired level of support
(3) Explanations for answers to the previous question
Yes:
- Has supportive loved ones and / or colleagues
- In therapy or seeing a psychiatrist
- Has financial support to access resources
- Lots of self-work: Engaged a lot with self-help, self-reflection, meditation, or tools one can use to improve their situation
- Doesn't feel the need to access support at the moment
- Regularly practicing meditation and mindfulness
Reasons for answering "Partly":
- Don't feel they need much support
- Haven't previously prioritized mental health / feels they don't have time to prioritize mental health
- Not good at implementing the help they get / has a hard time following up with resources that might be helpful to them (due to pre-existing conditions in a few cases)
- Feels they would benefit from having a little more structure in their mental health routine
- Don't know what kind of support they need, or don't know where to begin searching for it
- Experiences decision paralysis
- Not sure of how to access what they're interested in (e.g. internal family systems, psychedelics)
- Hard time describing what they're going through and putting words to what they need
- Feeling unconnected, unseen, and / or like no one understands
- Feeling like people are generally apathetic
- Has a hard time connecting to others and opening up to them
- Feels they need to have more open and honest conversations with their community to not feel alone and learn from others
- Currently looking for new perspectives and advice
- Feels they get good support, except among their interactions with members of the Effective Altruism community, which have generally been substantially harmful to their well-being
- Feels that Effective Altruism is scary due to too much existential dread. Talking with real people helps calm them now, but when it's just them and their laptop, engaging with Effective Altruism can feel overwhelming.
- Feels they get enough social support, but that there are not enough community-level interventions
- Feels supported by close friends and family, but not in ways they find practically helpful most of the time
- Feels supported too feel good, but not necessarily to flourish
- Support they're receiving is not as helpful as they'd have liked
- Feels social support network is not very supportive, but unsure of what additional forms of support they'd like from it / Feels they need more support but like they can't ask for it
- Relocated / Relocating and trying to build a new support network
- Thinks they should probably start therapy, but not sure with therapeutic method would be best, or they're in therapy, but not sure the method they're trying is right for them
- Hard to find they help they need (therapy, psychiatry, support networks they feel they can open up to), or on a waitlist for the help they're seeking
- Feeling "unqualified" to access support through the Effective Altruism community due to not working on EA projects
- Lack of financial resources to get the support they need
- On antidepressants, but feels as though the underlying issues aren't being addressed
- Potentially too high of expectations of themselves and what they can humanly do in a day
- Feels they need help structuring their lives to be optimally productive, and would like to find a role that makes better use of their innate talents, skills, and abilities
- Would like to be able to switch off from work more often, without feeling guilty about it
- Needs an accountability system
- Wants to hear more about supplements and other mental health initiatives
- Nutrition deficiencies - could benefit from more information on nutrition
- Would like to know more about interventions to help with feeling more clam and less anxious, and to be able to think more clearly and focus
- Feels they need more evidence-based resources
- Feels there is a need for better, more competent mental health institutions and government support
- There needs to be more discussion about mental health and emphasis on mental health resources in Effective Altruism, and in general
Reasons for answering "No":
- Feel they can manage on their own, or don't need or want support
- Can't find a good therapist
- Put off by cost of therapy
- Anxiety about reaching out to people for support
- Lack of social opportunities
- Feeling like no one cares
- Difficulty connecting with others
- Would like information about how to proactively improve their health, well-being, and productivity / performance that is accessible (especially as it concerns food and supplements)
(4) Support formats people would like to try
Please note: People who answered this question could provide multiple answers.
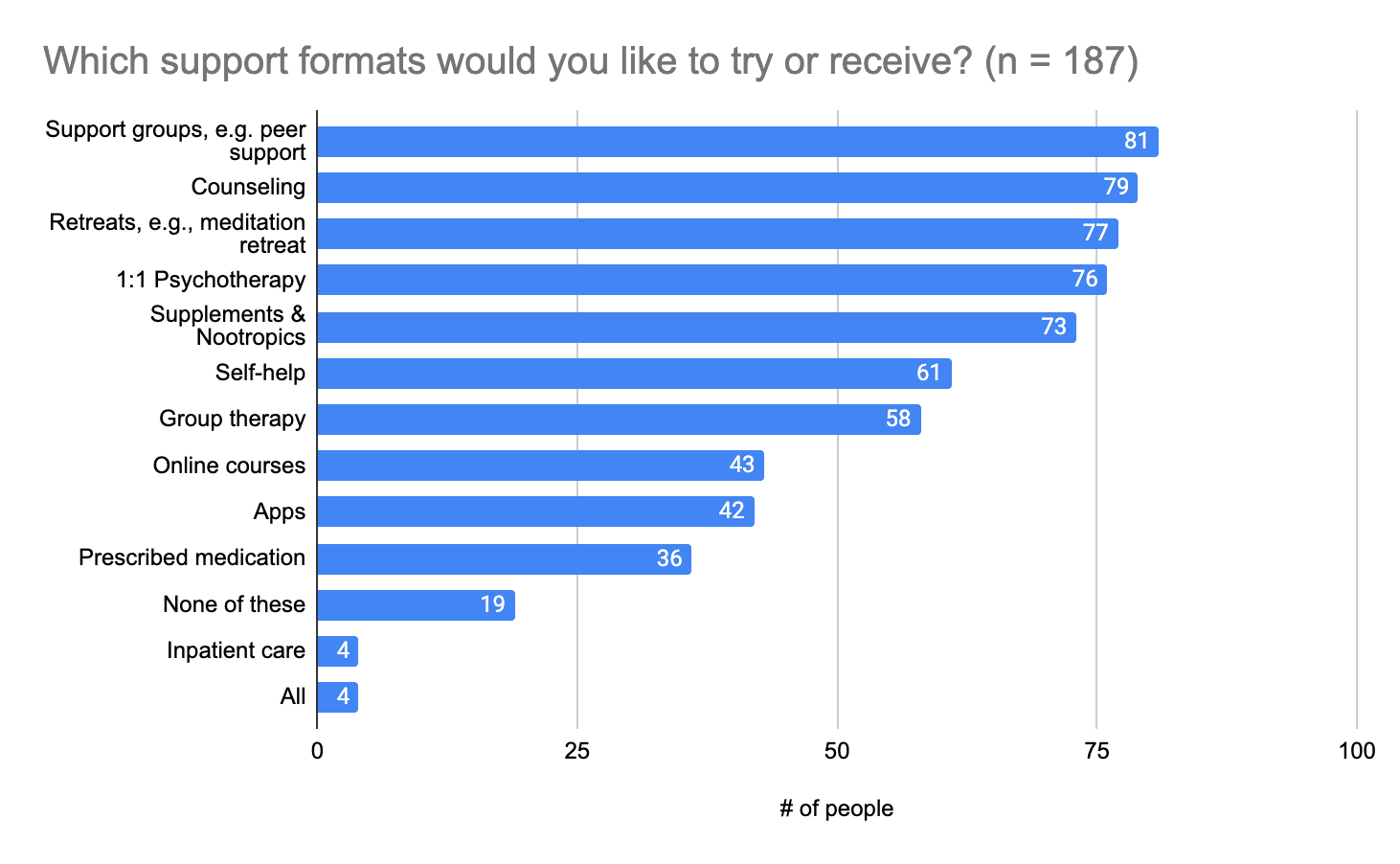
Other answers that were provided were:
- Coaching
- Matchmaking to people who want marriage and kids.
- Social events and gatherings
- Worksheets, guides, summaries of evidence (including populations, evidence quality, etc., similar to Examine but for interventions in addition to supplements)
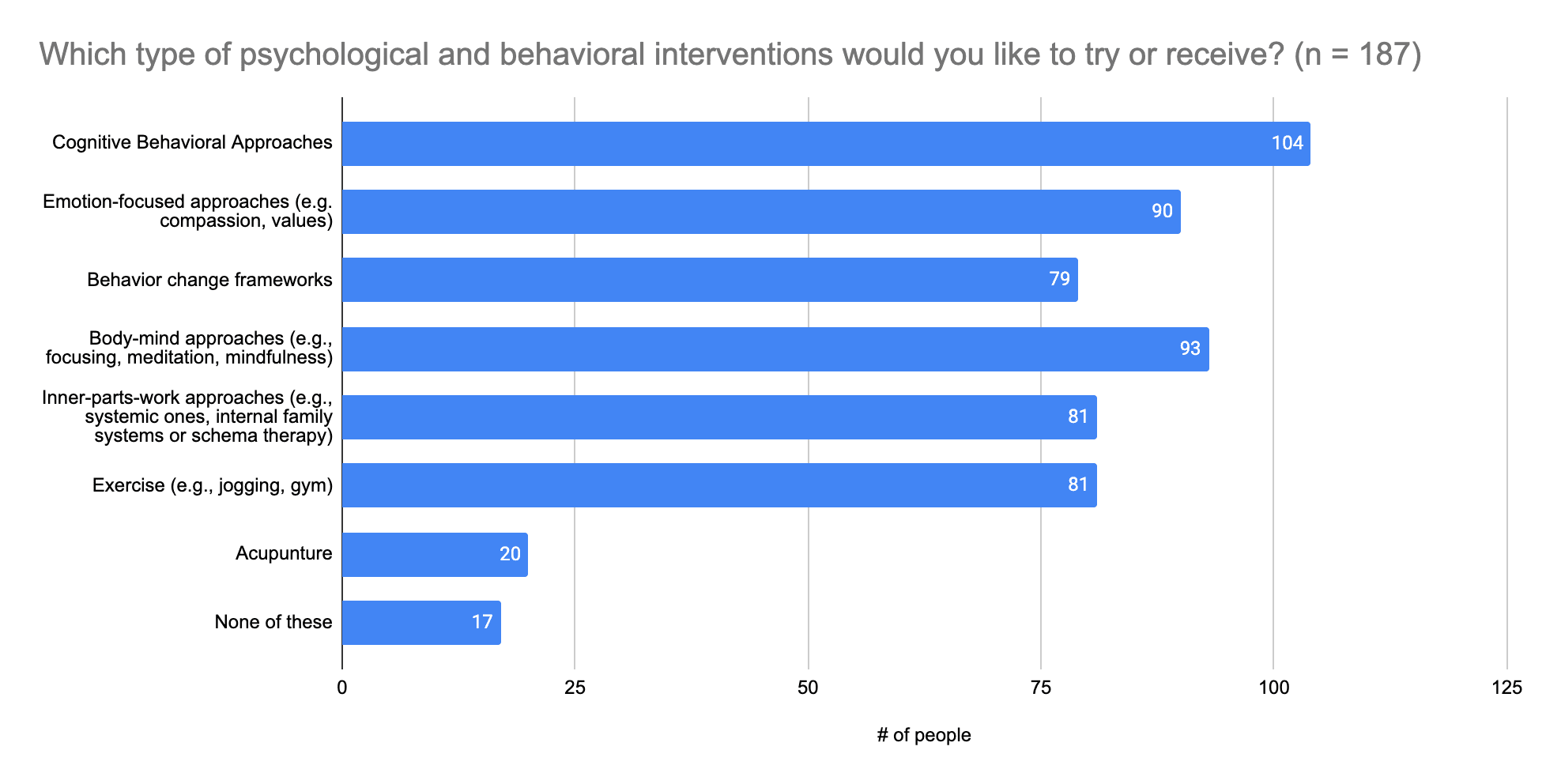
(5) Psychological and behavioral interventions people would like to try
Please note: People who answered this question could provide multiple answers.
Categories of psychological and behavioral interventions provided were (top to bottom of the chart):
- Cognitive Behavioral Approaches
- Emotion-focused approaches (e.g. compassion, values)
- Behavior change frameworks
- Body-mind approaches (e.g., focusing, meditation, mindfulness)
- Inner-parts-work approaches (e.g., systemic ones, internal family systems or schema therapy)
- Exercise (e.g., jogging, gym)
- Acupunture
Other answers provided were:
- More talking about how perception/thinking works for others (e.g. getting "nothing" from a body scan is called "numbness")
- Nofap, organizational methods
- More woo-woo/niche psycho-technologies, e.g. Reiki
Types of therapy people emphasized as of interest or previously helpful:
- Compassion Focused Therapy
- Acceptance and Commitment Therapy (ACT)
- Psychodynamic Therapy
- Dialectical Behavior Therapy (DBT)
Some people were not sure about how to respond to this question, because they didn't know what all of the options were or entail.
(6) Drugs people would like to try
Please note: People who answered this question could provide multiple answers.
Categories of drugs were (top to bottom of the chart):
- Psychedelics
- Stimulants except for caffeine (e.g. Adderall / Amphetamine, Ritalin / Concerta / Methylphenidate)
- Antidepressants (e.g., SSRIs, SNRIs, NRIs)
- Mood stabilizers (e.g. Lithium, etc.)
- Anxiolytics (e.g. Diazepam, Lorazepam, etc.)
- Antipsychotics
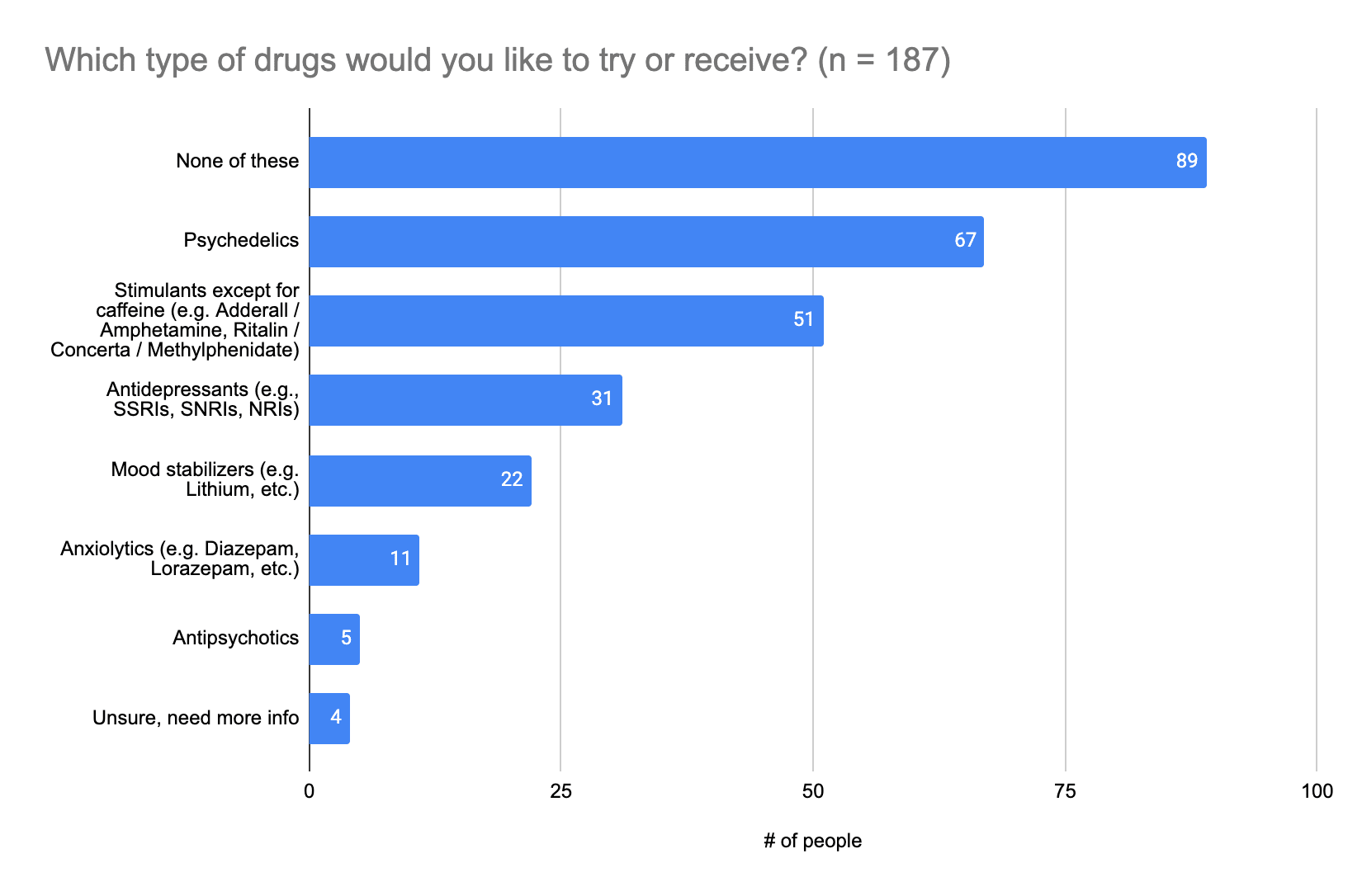
Other answers provided:
- Beta blockers for performance anxiety around interviews, public speaking, etc.
- Sleep aids, vitamins, melatonin
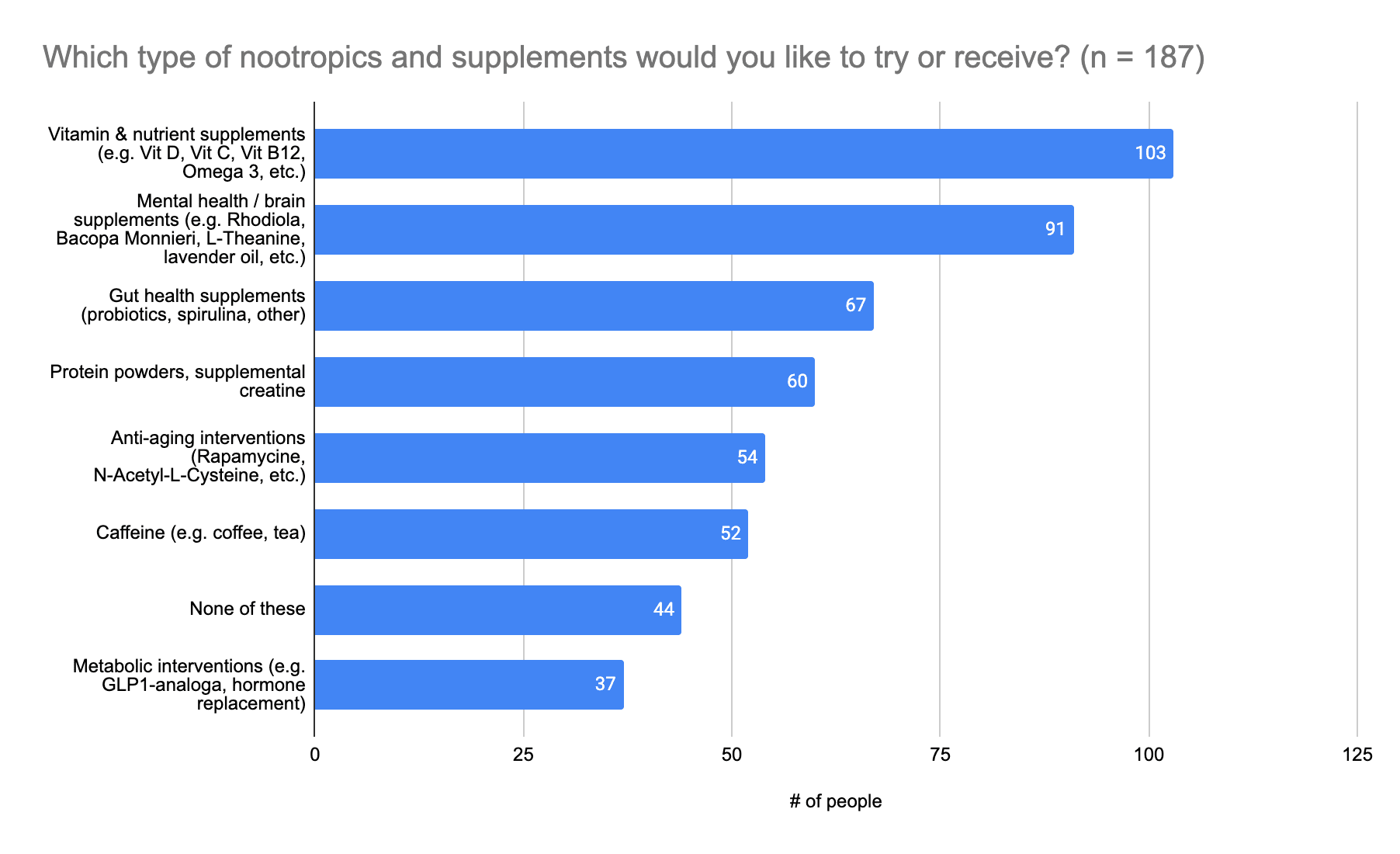
(7) Types of nootropics and supplements people would like to try
Please note: People who answered this question could provide multiple answers.
Categories of nootropics and supplements were (top to bottom of the chart):
- Vitamin & nutrient supplements (e.g. Vit D, Vit C, Vit B12, Omega 3, etc.)
- Mental health / brain supplements (e.g. Rhodiola, Bacopa Monnieri, L-Theanine, lavender oil, etc.)
- Gut health supplements (probiotics, spirulina, other)
- Protein powders, supplemental creatine
- Anti-aging interventions (Rapamycine, N-Acetyl-L-Cysteine, etc.)
- Caffeine (e.g. coffee, tea)
- None of these
- Metabolic interventions (e.g. GLP1-analoga, hormone replacement)
Summary of Results
Most survey participants are interested (n = 125; 67%) or at least somewhat interested (n = 47; 25%) in learning more about and using interventions that could help them improve their health, well-being, and productivity or performance. About a quarter of survey participants feel they are getting the support they need or want (n = 49; 26%), but most feel that’s only partly true (n = 112; 60%), so there’s definitely room for improvement. Reasons for people feeling they are only partly receiving the support they need vary, but a common trend appears to be a need for help with mental health routines, priorities and structure, and help with feeling comfortable understanding and communicating what one is feeling and needs, and finding people with whom one is comfortable discussing those feelings and needs.
The top five support formats survey participants are interested in trying are support groups (n = 81; 43%), counseling (n = 79; 42%), retreats (such as meditation retreats (n = 77; 41%), 1:1 psychotherapy (n = 76; 41%), and supplements and nootropics (n = 73; 39%). People are also generally interested in trying all of the behavioral and psychological interventions listed (n = 79+; at least 42%), with the exception of acupuncture.
In terms of drugs, a lot of people would like to try psychedelics (n = 67; 36%) and stimulants (n = 51; 27%), and in terms of nootropics and supplements, there’s a lot of interest in trying vitamins and nutrient supplements (n = 103; 55%), as well as mental health / brain supplements (n = 91; 49%).[1]
Important Factors for Intervention Use Decisions
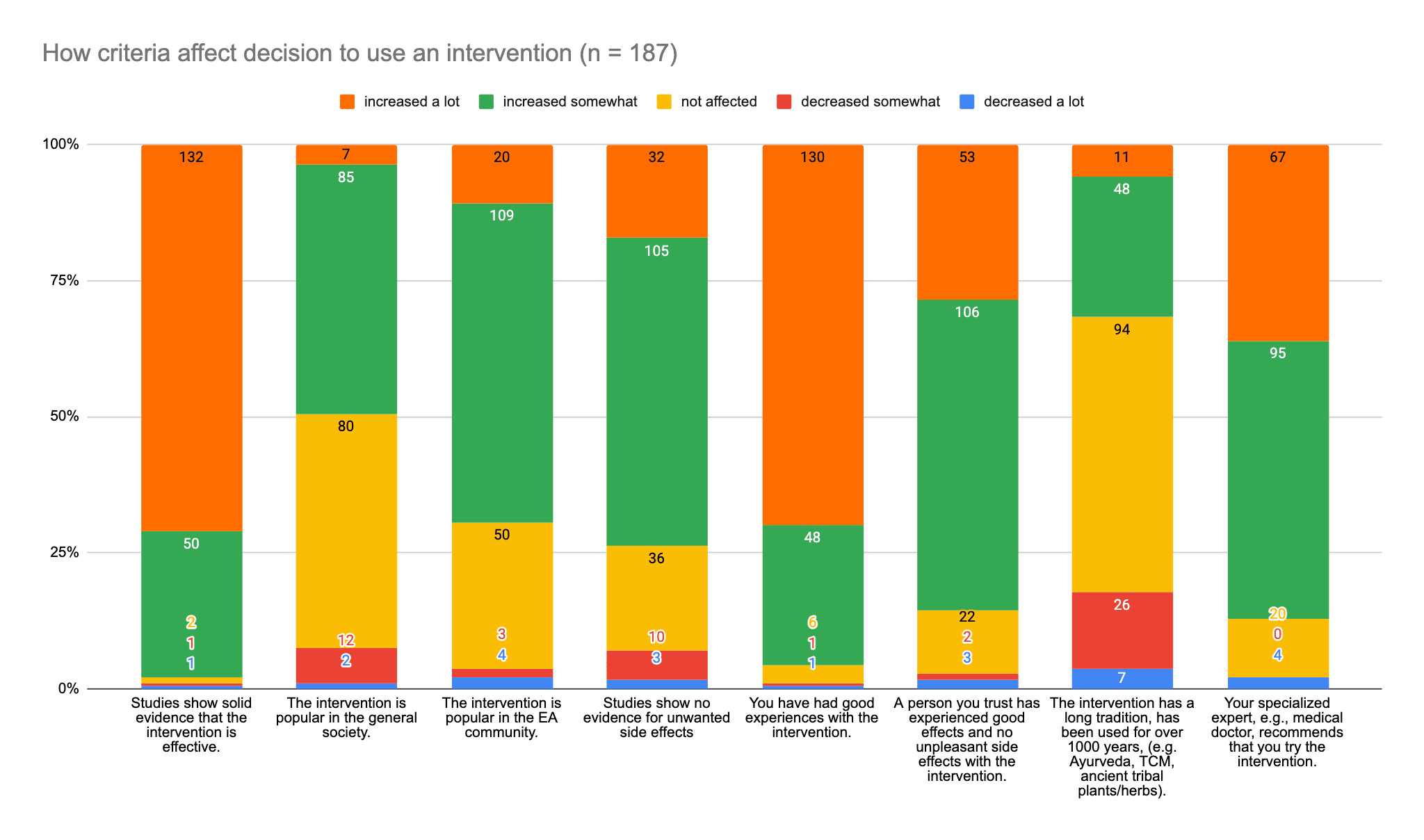
(1) How do the following criteria affect your decision on whether to use an intervention to improve your mental health or productivity?
The answer was provided by selecting the missing word in the sentence “The likelihood of me using an intervention is ... by this criterion.”
Answer options were:
- Increased a lot (orange in the chart)
- Increased somewhat (green)
- Not affected (yellow)
- Decreased somewhat (red)
- Decreased a lot (blue)
Criteria were as follows, and are provided as column labels from left to right:
- Studies show solid evidence that the intervention is effective.
- The intervention is popular in the general society.
- The intervention is popular in the EA community.
- Studies show no evidence for unwanted side effects.
- You have had good experiences with the intervention.
- A person you trust has experienced good effects and no unpleasant side effects with the intervention.
- The intervention has a long tradition, has been used for over 1000 years, (e.g. Ayurveda, TCM, ancient tribal plants/herbs).
- Your specialized expert, e.g., medical doctor, recommends that you try the intervention.
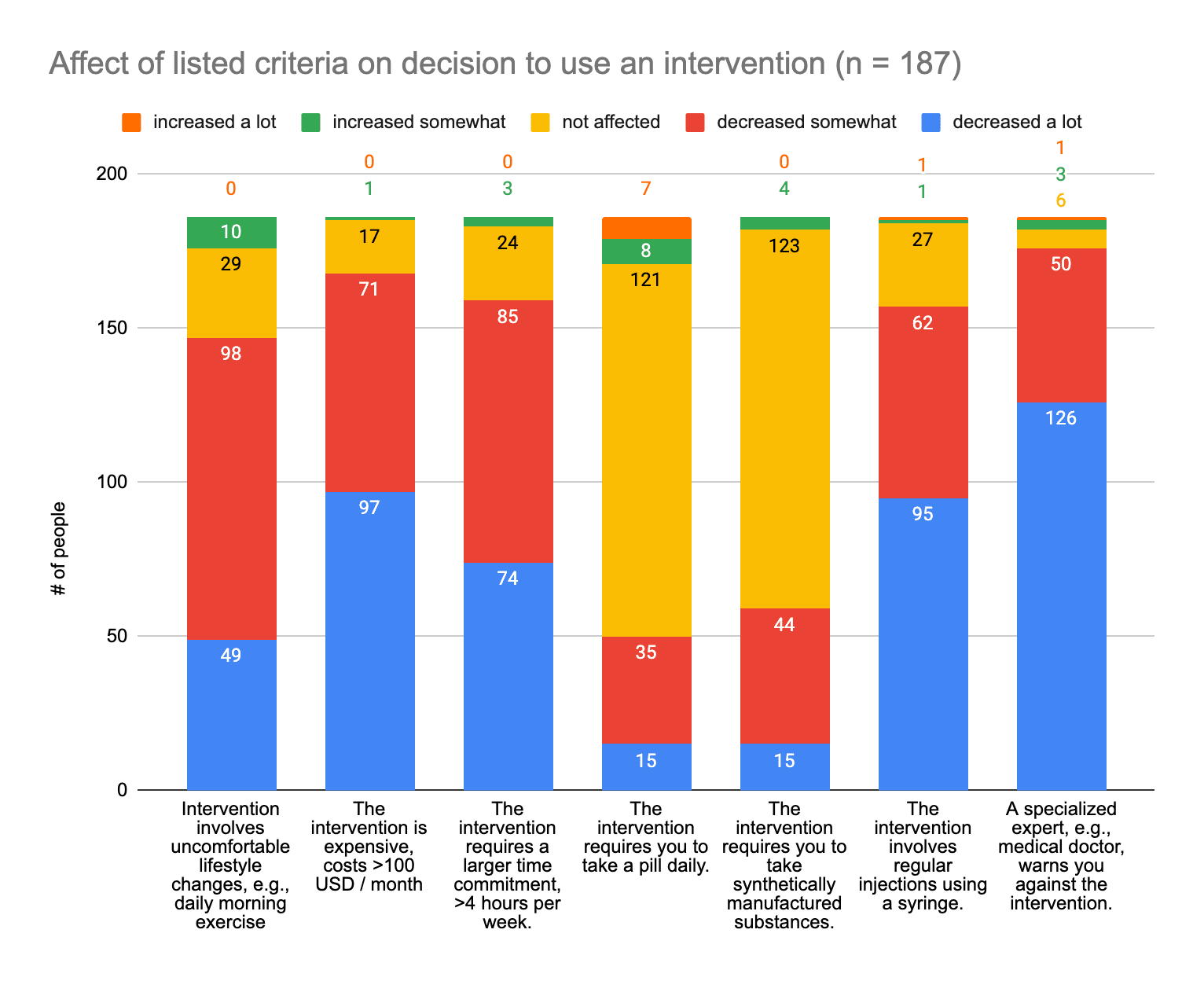
(2) How do the following criteria affect your decision on whether to use an intervention to improve your mental health or productivity?
The answer was provided by selecting the missing word in the sentence “The likelihood of me using an intervention is ... by this criterion.”
Answer options were:
- Increased a lot (orange in the chart)
- Increased somewhat (green)
- Not affected (yellow)
- Decreased somewhat (red)
- Decreased a lot (blue)
Criteria were as follows, and are provided as column labels from left to right:
- Intervention involves uncomfortable lifestyle changes, e.g., daily morning exercise
- The intervention is expensive, costs >100 USD / month
- The intervention requires a larger time commitment, >4 hours per week.
- The intervention requires you to take a pill daily.
- The intervention requires you to take synthetically manufactured substances.
- The intervention involves regular injections using a syringe.
- A specialized expert, e.g., medical doctor, warns you against the intervention.
Please note: Numbers above the chart are associated with the color groups in the respective columns.
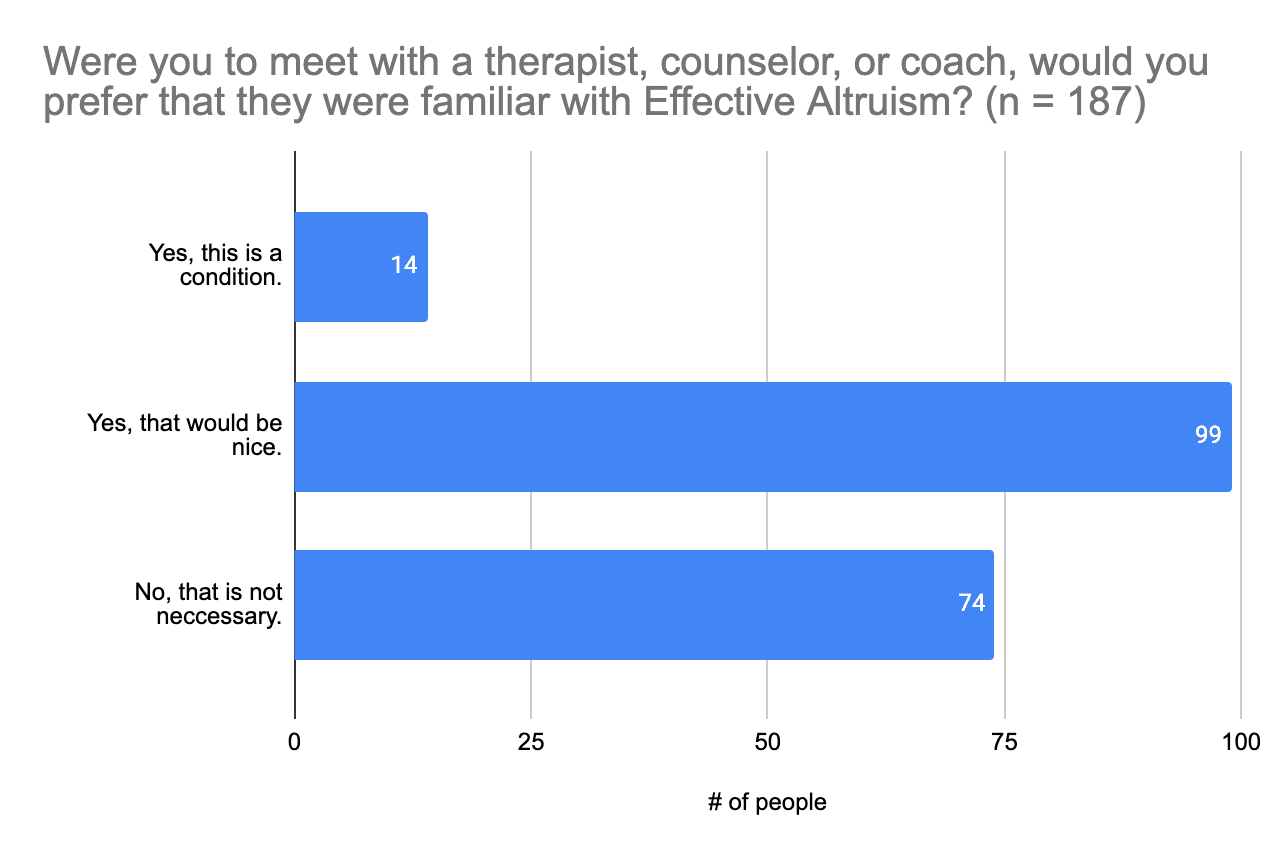
(3) Preference for a therapist, counselor, or coach familiar with Effective Altruism
Most people (n = 99) think it would be nice to meet with a therapist, counselor, or coach familiar with Effective Altruism, but that is not something they require to receive mental health support, and for many people it is not necessary at all (n = 74).
Summary of Results
Studies that show solid evidence that an intervention is effective and good experiences with an intervention are the two factors that have a lot of influence over 50% of survey participants’ decisions to use a given intervention. For more than half of participants, decisions were somewhat affected by the popularity of the intervention (n = 109; 58%), studies showing no evidence of unwanted side effects (n = 105; 56%), a person they know having good experiences and no bad experiences with the intervention (n = 106; 57%), and a specialized professional, such as a medical doctor, recommending the intervention (n = 95; 51%). Survey participants are less likely or far less likely to use an intervention if a specialized professional warns them against it (n = 176; 94%), it involves regular injections (n = 157; 84%), it requires a larger time commitment (i.e., >4 hours per week) (n = 159; 85%), it’s expensive (> $100 (USD) each month) (n = 168; 90%), or it involves uncomfortable lifestyle changes (n = 147; 77%). So interventions ideally need to be certified by professionals, involve little commitment in terms of time and money, and not have large effects on people’s lifestyles. And for the majority of survey participants (n = 173; 93%), they do not necessarily need to be provided by therapists, counselors, or coaches familiar with Effective Altruism.
Conclusion
Members of the Effective Altruism community who participated in this survey are generally satisfied with their lives (70%) and the level of support they receive (63%), but they could do with and are open to trying a range of interventions that could help them improve their mental health and productivity, especially as it concerns anxiety, depression, and ADHD; improving one’s concentration, attention, focus, and productivity; and overcoming procrastination. Furthermore, there appears to be a need for help with mental health routines, priorities and structure, and help with learning to communicate what one is feeling and needs.
As far as behavioral and psychological interventions are concerned, there’s interest in trying to learning more about cognitive behavioral approaches, emotion-focused approaches (e.g., compassion, values), behavior change frameworks, body-mind approaches (e.g., focusing, meditation, mindfulness), inner-parts-work approaches (e.g., systemic approaches, internal family systems or schema therapy), and exercise. As it pertains to substances, people are generally interested in trying psychedelics, stimulants, vitamins and nutrient supplements, mental health / brain supplements.
A lot of other interesting ideas and suggestions were made via the free-form responses in this survey as well, so please do take a look at those if you are looking for inspiration.
Limitations of These Survey Results
These survey results are likely limited by selection bias. It is likely that more people who are struggling with mental health than those who are not have taken part in this survey. For this reason, this survey does not allow us to make statements about how prevalent things are in the community but only how prevalent they are among those interested in mental health and productivity. This bias was additionally fed by a distribution bias, as this survey, though advertised in common places such as the EA Forum and the large EA Facebook group, was also heavily advertised in EA circles with an interest in mental health and productivity.
Acknowledgements
A big thank you to everyone who participated in the 2023 EA Mental Health & Productivity Survey! Your answers will help us and others in the community provide mental health resources and information on resources more suited to your needs and interests.
Author Contributions
Emily Jennings (Mental Health Navigator), Inga Grossmann (Rethink Wellbeing), and Tim Farkas designed this survey in December 2022. Tim Farkas and Samuel Nellessen contributed questions concerning productivity and substances, and Tim Farkas provided feedback on the survey design. Emily wrote up the results in May and June 2023, and Inga reviewed the draft and added sources, calculations, and a few reflections.
Data Availability Statement
The anonymized data generated and analyzed (with the exception of responses to open-ended questions) are available upon request to the Mental Health Navigator at info@mentalhealthnavigator.co.uk for those who might wish to do follow-up analyses.
Feedback & Comments
We’d be happy for you to reach out and leave constructive comments and suggestions to make us and readers aware of and discuss:
- Any additional insights and interpretations you might have;
- Potential limitations of the results;
- Anything you feel might be interesting to include or do differently for a potential next edition of this survey.
If you feel more comfortable sending your suggestions or comments by email, feel free to send them to the Mental Health Navigator at info@mentalhealthnavigator.co.uk.
We might add to the report or update for a more polished version later on. If you’d like to support this effort or help run the next EA Mental Health and Productivity Survey, please let us know via contact@rethinkwellbeing.org.
- ^
Please note that we do not encourage the use of anything illegal.
Thanks for putting this together!
At a glance, it looks like this broadly matched the demographics of the broader EA Survey, except for gender (women were dramatically over-represented in the mental health survey) and engagement (people who took the mental health survey were much more highly engaged).
I agree with you that this survey will also very likely select for people with more of an interest in mental health and perhaps suffering from mental health issues. I imagine this might explain the relatively low life satisfaction you found:
I'd just like to say that I had OCD/GAD for ~ 10 years but now have no symptoms due to lifestyle changes and therapy. If anyone would like to chat with me about this I'm very happy to chat yannikyriacos@gmail.com
if a third party ran the survey, the results would be similar? Did you take any measures to prevent a “an EA org is running this so I have to adjust my answers accordingly” bias?