I volunteer with a small community-based project in Lucknow, which helps support tuberculosis (TB) patients in accessing healthcare. India has the ambitious goal of ending TB by 2025 – but we are currently a long way off, with over 2.8 million cases and 340,000 deaths annually. The government needs to make much greater efforts to actively find ‘missing’ TB cases and ensure all TB patients receive treatment - and adequate nutrition.
To this end, I have reviewed some of the literature and compiled a set of five policy proposals that can make a significant contribution to tackling the epidemic:
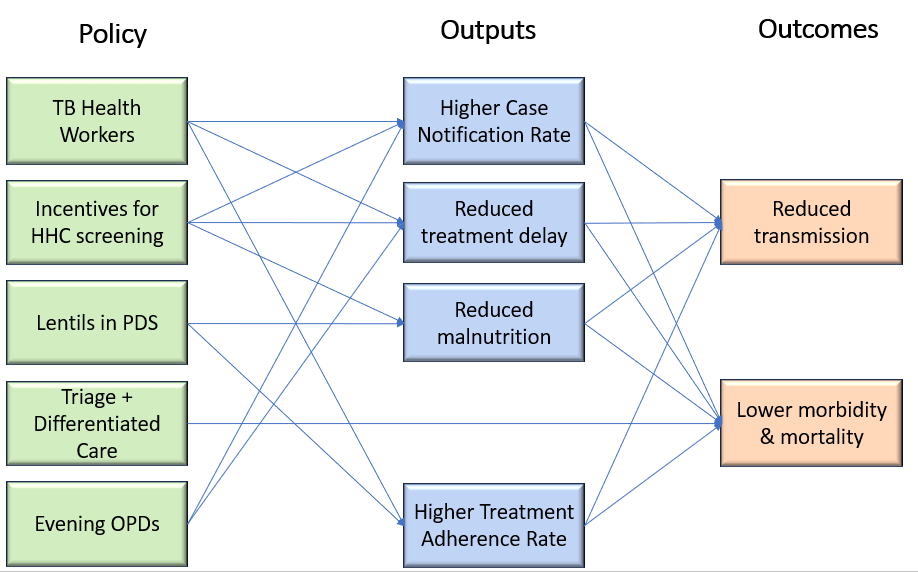
- Employing community-based TB workers with a mandate of TB case finding and patient support.
- Giving small incentives to encourage household contacts of TB patients to get screened and take Tuberculosis Preventative Treatment (TPT).
- Triaging TB patients at point of diagnosis, and hospitalising those most at risk of adverse outcomes.
- Providing free lentils to households of TB patients through the public distribution system, to improve nutrition.
- Conducting evening OPDs in government hospitals to enable poor households to seek healthcare more convenient.
This draft report shares these policy proposals in more detail, as well as cost-efficacy analyses, literature reviews, and stories from the field. You can find the spreadsheet with cost-efficacy calculations here. If you want to leave comments on the report, here is the google doc version (less visually attractive).
My rough calculations indicate that the policies have cost-efficacy around US$100 per DALY averted – competitive with top GiveWell charities. While implementing these policies would require roughly 32 billion INR (nearly USD 400 million) per year, they would avert some 4 million DALYs.[1]
I would appreciate feedback and suggestions: on any of these policy ideas, on other ideas we should include, on any improvements in the analysis.[2] If you would like to be more heavily involved in this project, I am looking for co-authors to collaborate with - please drop a comment below. Ultimately, we want to be part of a coalition to approach relevant state and national authorities and advocate for piloting some of these policies.
- ^
The current National Tuberculosis Elimination Program is only about 31 billion INR. The fact that these five highly cost-effective policies, which would require a doubling of the TB budget, are projected to avert only 13% of India's DALYs lost due to TB is a stark indication that the government is not spending nearly as much as required to come even close to ending TB.
- ^
One particular methodological question I’m curious about is how best to factor in the indirect effects when dealing with an infectious disease like TB. That is, averting one case of TB now (e.g. through better nutrition) is likely to avert some number of future cases who would have been infected from that index case. I couldn’t find much in the literature on this, but ended up going for Shrestha et al’s model, which dealt with active case finding in a medium sized Indian city. Shrestha found that their proposed intervention averted 81 deaths (directly) in Year 1, and 143 deaths (indirectly) in Years 2-10, giving a ratio of approximately 1 : 1.8.


Yep... this stuff is simultaneously fairly obvious and surprisingly neglected. I have been looking at TB programs in various developing countries and the best policy proposals all include these components - although the details differ in some places. Implementation is a challenge.
I've been paying special attention to household contacts screening for TB and preventative treatment (TPT; your policy #2). While TPT for household contacts is extraordinarily cost-effective, it is quite frustrating to make progress on this, because of the reasons the report cites: general lack of awareness of TB dangers, as well as that it is quite hard to convince people who are not visibly sick to travel with their family, possibly long distances, to hospitals to get screened and take 3-month courses (or longer!) of preventative antibiotics with sometimes-severe side effects.
Glad to see more people working on this.